Chapter 4 - Unmet needs
The CSTDA has specified the shared responsibility of governments
in making demand adjustments. It is the view of the Office [of the Public
Advocate] that the incremental increase in resources that has been provided
through the CSTDA is no longer sustainable. There is truly a crisis of unmet
need for services and support for people with disabilities, their carers and
families. There needs to be a significant injection of additional resources to
address the unmet need that has been endemic in the system for the life of the
CSTDA.[1]
4.1
Unmet need for disability services has been an issue for many years.
Service providers, support and advocacy groups and individuals can provide countless
instances where a person with a disability either has had no access to the services
they require or has access to services which meet their needs only to a limited
extent. The areas where needs are not being met include accommodation services,
respite services, in-home care and supply of equipment and aids. A range of
studies provide estimates of the level of unmet need including Australian
Bureau of Statistic (ABS) surveys and reports from the Australian Institute of
Health and Welfare (AIHW). These are discussed below.
4.2
Unmet need became a priority for government under the second CSDA with
the Commonwealth offering the States and Territories $150 million over the last
two years of the Agreement to help the States and Territories address unmet
need for services. The Commonwealth provided the additional funding on the
proviso that the States and Territories contributed a similar amount. The
States and Territories contributed $366 million over the two years. The
Commonwealth continued the funding in the third Agreement.[2]
4.3
Under Bilateral Agreements with the Commonwealth in 2000, all
jurisdictions were funded to 'help address unmet needs by providing additional
services which enable people with disabilities who have ageing carers to remain
supported within their families in their local communities'. The Bilateral
Agreements also noted that the 'State's contribution will be used to assist in
addressing other priority areas of unmet need'. These other priority areas were
not specified in the Bilateral Agreements. The effectiveness of the unmet need
funding was evaluated in 2002 by the AIHW. This is discussed below.
4.4
Even with this substantial additional funding, significant levels of
unmet need remain. State and Territory Governments argue that they lack the
capacity to provide further resources. The Commonwealth, while acknowledging
there is still a level of unmet need, has stated that the 'data collected and
made available by the States and Territories does not allow an accurate
assessment of the level and nature of this need'.[3]
4.5
The Committee does not accept this buckpassing between jurisdictions and
considers that a much greater and better-resourced effort is required to
address unmet need by all jurisdictions.
Disability support services
4.6
Services provided under the CSTDA are targeted at people with a need for
ongoing support in everyday activities and aim to 'maximise the opportunity for
people with disabilities to participate socially and economically in the
community'. The 2002-2007 Agreement specifies that a disability experienced by
a CSTDA service user should be manifest before the age of 65 years. The AIHW
noted that services do not generally place upper age restrictions on their
clients.
4.7
National data on services provided under the CSTDA are collected through
the CSTDA National Minimum Data Set (NMDS). The following provides a brief
overview of the size and scope of the disabled population in Australia and the
utilisation of services for 2004-05:
- approximately 4 per cent of the population (697,124 people) aged
less than 65 years have the potential to require CSTDA-funded services at
some time;
- 200,493 service users accessed CSTDA-funded services during
2004-05;
- 46 per cent of service users accessed community support, 32 per
cent employment services, 22 per cent community access, 17 per cent
accessed accommodation support services, 12 per cent accessed respite services;
- 41 per cent of CSTDA service users had an intellectual
disability;
- 3.1 per cent of CSTDA service users were identified as being of
Aboriginal or Torres Strait Islander origin;
- around 18 per cent of CSTDA service users reported that they
received individualised funding with those in respite and employment services
most likely to report that they received such funding;
- 29 per cent of users accessed services from two or more
CSTDA-funded service groups; and
- 42 per cent of users indicated that they had an informal carer.[4]
Assessments of unmet need
4.8
In 1998 the ABS Survey of Disability, Ageing and Carers showed that
956,600 people with a profound or severe disability needed assistance with the
core activities of self care, mobility and/or communication. The major
proportion of these (97 per cent) received some assistance to meet their need
for help with core activities with 57 per cent indicating that they had their
need for assistance fully met, 40 per cent needed more help than they actually
received and 3 per cent (24,400) received no help at all. For carers, the ABS
indicated that 42 per cent of primary carers did not need any assistance,
25 per cent of primary carers did not get enough help and 9 per cent of
primary carers who needed help did not receive any assistance.[5]
4.9
The AIHW has published a number of reports on the demand for disability
services. In 1997, the AIHW reported on a study to provide estimates of unmet
demand for accommodation and support, respite and day programs, the cost to
government of meeting unmet demand and project growth in demand for specialist
disability services.
4.10
The AIHW estimated that in 1996 there were 13,400 people aged 5-64 years
who experienced an unmet need for accommodation, support and respite services.
There was also an unmet demand by an estimated 12,000 people (or
full-time-equivalent places) for day programs in 1996. The AIHW commented that
these estimates for accommodation and support and respite were considered to be
conservative because the estimates excluded certain groups including those in
'health establishments' (some 19,000 in 1993 in hospitals, nursing homes and
other institutions) and children under 5 years of age and because growth
factors were placing ongoing pressure on services, chiefly the ageing of
clients and their carers. Day program estimates were also considered to be
conservative for several reasons including that they excluded certain groups
such as people with severe handicap who needed assistance sometimes rather than
always and people who were employed part-time; it was assumed that there was no
growth in total demand since 1993; and no additional services were offered to
current program users.[6]
4.11
The AIHW concluded that projected demographic trends, particularly
population ageing, would result in a substantial projected increase in the
number of people in the CSDA target group for the period 1997-2003. The ageing
of carers was seen as continuing to be an important issue, while the ongoing
trends in de-institutionalisation would continue to place pressure on families
and community-based services.[7]
4.12
In 2001 the National Disability Administrators (NDA) commissioned the
AIHW to update the 1997 report, to examine the effectiveness of the unmet need
funding provided to States and Territories in the last two years of the second
CSDA and to estimate any remaining shortfalls. The AIHW reported in 2002 and
found that the unmet need funding had been effective in putting services on the
ground.[8]
Those services which focused on flexibility, the use of individual packages and
local area coordination mechanisms were viewed positively.
4.13
However, the AIHW reported that quantifying or tracking the use of the
additional services resulting from the unmet need funding was not easy. The
AIHW found that jurisdictions differed in the application of the unmet need
funding, the speed and method of the rollout, the information they could
provide and the extent to which the unmet need funding and its application were
identifiable in administrative systems and processes. Information requested by
AIHW in its survey of jurisdictions could not be provided by all jurisdictions.
In addition, the Bilateral Agreements were not accompanied by consistent
agreements about acquittal and reporting to the Commonwealth and some of the
reporting agreements had not yet been fulfilled.
4.14
The AIHW concluded that the full impact of the new funding would not be
apparent in client outputs until 2002-03. As to unmet need in 2001, the AIHW
estimated that:
- 12,500 people needed accommodation and respite services;
- 8,200 places for community access services were needed; and
- 5,400 people needed employment support.[9]
4.15
The AIHW stated that it had made these estimates on a conservative
basis, with the aim of providing reliable 'lower bound' estimates. In addition,
the estimates did not represent the sum total of unmet need for CSDA services
as community support services were not included in the project brief. Other evidence
also suggested further unmet need:
- some 5,300 older carers in the target group of the Bilateral
Agreements had either never received respite and wanted it, or had received it
in the previous three months and wanted more;
- most new services were provided to people with urgent needs;
- there appeared to be between 6 and 24 times more people seeking
services and on jurisdiction registration or waiting lists in 2000-01 than were
removed from these lists; and
- anecdotal evidence pointed to community knowledge of waiting
lists was possibly dampening the numbers of applications.
4.16
The AIHW again identified a range of issues which suggested that the
overall service system for people with disabilities was under pressure. These
issues included the ageing of the CSDA broad target group; the number of people
with disability aged under 65 years living in residential aged care; the high
numbers of people with disabilities using services for the homeless; transport
needs are not part of disability services; and systems for the provision of
equipment appear to be nationally fragmented.
4.17
In addition to the AIHW's comments on the conservative nature of its
estimates other witnesses pointed to shortcomings in the estimation of unmet
need. ACROD noted that the AIHW study did not consider under-met need or needs
being inappropriately met.[10]
The National Council on Intellectual Disability argued that the full extent of
unmet need will never be known as most States and Territories do not keep waiting
lists or needs registers and 'therefore it becomes impossible to determine how
many people need support and what they need support for'.[11]
4.18
Witnesses also noted that a people funded under a range of insurance and
compensation schemes for injuries or disabilities arising from motor vehicles
or work accidents and people with disabilities receiving funding through the
Department of Veterans' Affairs sit outside the CSTDA arrangements. In
addition, people with disabilities who receive damages obtained through the
courts under public liability actions are funded independently of any
Commonwealth, State or CSTDA funding arrangements. Ms Raelene West commented
that the failure to include these disability services within the structure of
the CSTDAs has 'distorted the view of how disability service delivery is truly
funded (or not funded) across Australia, failing to provide an adequate picture
as to many inequities in funding that exist across the entire disability
sector, not just within the CSTDA arrangements'.[12]
4.19
In 2005, the AIHW was commissioned to update its analysis of unmet need.
The AIHW indicated that the final report was due at the end of February 2007.[13]
Disability services data
...we do not have reliable data about the level of need. We know
it is massive and that it is growing, but we simply cannot identify accurately
enough to project what we need to do in the future.[14]
4.20
At the core of any analysis is the reliability of the data used. In the
context of disability services, the difficulties of obtaining reliable and
comparable data from eight jurisdictions have been acknowledged and
improvements have been undertaken.
CSDA Minimum Data Set
4.21
Following the signing of the first CSDA, the AIHW was requested to
assist in the development of an agreed Minium Data Set (MDS) for CSDA-funded
services. The AIHW noted that while the need for relatable data on disability had
been recognised for some time, there were major difficulties in bringing the
data together including the use of varying definitions and terminology.
4.22
The MDS was developed as an agreed set of data items and for each data
item an agreed definition to be applied across all CSDA-funded services. From
1994, the CSDA Minimum Dataset provided funding bodies, funded agencies
(service providers), service users and other stakeholders with information
about services delivered under the CSDA and the people receiving those
services. The information was collected on one snapshot day in the year.
CSTDA National Minimum Data Set
4.23
In 1999, the NDA and the AIHW undertook a review and redevelopment of
the CSDA MDS collection. The redeveloped collection, referred to as the CSTDA
National Minimum Data Set (NMDS), was fully implemented nationally in October
2002. The first collection period for the CSTDA NMDS was for the six months
commencing on 1 January 2003.
4.24
The CSTDA NMDS has an agreed set of data items of national significance
and an agreed framework for collection. Data items relate to equity, efficiency
and effectiveness of services and is collected throughout the year from funded
agencies about all service users. Not all agencies provide the same level of
data: accommodation and community support services provide all data items
relating to service users whereas recreation or holiday program providers
provide only minimal information. Services such as advocacy and print services
are not required to provide service user details.
4.25
Items on informal carers were introduced in the CSTDA NMDS. This is in
recognition of the mutual support among people with a disability, informal
carers and formal services, and the fact that program goals are recognising, in
particular, the importance of ageing carers.
4.26
In specifying revised core data items for ongoing collection by all
service providers funded under the CSTDA, the CSTDA NMDS:
- aims to meet critical data needs across the disability field, and
to be consistent with other major data developments, such as the HACC MDS;
- integrates data collation with the operation of agencies and
funding departments;
- uses statistical linkage keys to enable data from various sources
to be related and collated without duplication; and
- uses statistical linkage keys to account for double counting of
service users.[15]
Improvements in datasets
4.27
The AIHW noted that disability data has improved and pointed to a number
of major developments:
- the National Aboriginal and Torres Strait Islander Survey 2002
provided information on Indigenous disability;
- the first full year of the redeveloped CSTDA NMDS collection
provided a new benchmark collection on disability services for future
reference;
- a disability question was included in the 2006 Australian Census;
- the AIHW is continuing to work on the implementation of the
International Classifications of Functioning, Disability and Health (ICF); and
- there is increasing adoption of national data standards, based on
the ICF, in administrative data collection.
4.28
The AIHW commented that these developments will provide improved
infrastructure for disability identification in generic services, enabling
access to, and outcomes from, these services to be monitored. Some of the
initiatives will be challenging, 'particularly when they involve bringing a
newer and more holistic conceptualisation of disability into the sphere of
health surveys and information systems and into the plethora of assessment
scales now used in human services fields in Australia'. The AIHW concluded
that:
The long-term vision is that, with more consistent approaches to
disability data across the spectrum of human services, the resulting 'joined
up' data will support whole-of-government approaches to the provision of
services relevant to people with a disability.[16]
4.29
In response to the Committee's invitation to indicate further areas of
improvement in data collection, the AIHW stated that:
...we do not have an incredibly good handle on what goes on within
some states. There seems to be a differential across states and territories in
terms of how well needs are met and how well even reporting is done. I think it
would be good to be able to ensure that, when we put the national together, we
are getting a true picture of what is happening within each of the
jurisdictions. We are pretty reliant on what is provided to us at a
jurisdictional level.[17]
4.30
The Report on Government Services 2006 addressed the issue of
data collection in the jurisdictions. It indicated that the implementation of
the CSTDA NMDS 'has led to some data quality issues'. In particular, the
proportion of service users and service outlets that provided data and the 'not
stated' rates of particular data items vary across jurisdictions.[18]
The Department of Families, Community Services and Indigenous Affairs (FaCSIA) also
noted inconsistencies in the way that service data is collected across
jurisdictions as some jurisdictions were unwilling to commit to the level of
data collection proposed prior to the last agreement. There is not a common
assessment platform across jurisdictions, which means the nature of the data
collected by services at the point of assessment also differs.[19]
4.31
The NSW Government noted that data collection response rates were poor
in NSW. The Government indicated that it was now assisting service providers to
return data and to improve the quality of the data including the use of
continuous electronic collection rather than a yearly census.[20]
4.32
ACROD commented on the need to improve data sets to guide and service
planning in order to make meaningful comparisons across jurisdictions. For
example, 2003-04 data suggest that community access expenditure per client
varies from $18,002 in NSW to $2,004 in Western Australia. ACROD commented that
at least some of this difference reflects variations in the response rates between
the States, the inclusion of disparate service models in the community access
category and varying hours of service per client.
4.33
ACROD concluded that the CSTDA should provide a planning framework for
the provision of disability services across Australia, one that takes into
account demographic changes, future service needs, the changing expectations of
service users and carers, the capacity of service providers and other relevant
factors. However, this planning framework will require an improvement in the
quantity and quality of data collected.[21]
4.34
Other shortcomings identified in the data collected included that it was
based on a 'one size fits all' mentality and collected data primarily around
personal care. As a result the specific needs of people who are blind or vision
impaired around mobility, transport and access to print are not collected at
all. Further, data is only collected from funded services and not from
organisations such as the Royal Society for the Blind which provide services
which are vital to independence.[22]
4.35
MS Australia noted that reporting has improved and pointed to the protocols
such as Quarterly Data Collection. However, currently the data collection
system used by CSTDA departments cannot discriminate between new entrants and
existing clients so there is no measure on how quickly waiting lists can be
cleared, or what happens to people while they wait. MS Australia also argued
that the data collection is aimed at addressing the Commonwealth's need for
accountability and that it does not measure the quality of the service
interaction or report any outcomes. MS Australia called for outcome measures,
including, but not limited to, counting the number of people serviced. MS
Australia concluded:
Decent planning cannot occur without good data, and the lack of
data is a major barrier to progress in the sector. There clearly needs to be a
better way of working out the future resourcing of disability services than
what individual Ministers can squeeze out of treasury year by year by year.
The next CSTDA should have mechanisms to measure the
jurisdictions performance on a number of outcome measures, including, but not
limited to counting the number of people serviced, numbers needing particular
services and an actuarial measure of the future demand and costs of the suite
of services from early intervention through to aged care.[23]
4.36
The Office of the Public Advocate Victoria also voiced concern about the
narrowness of the datasets:
While the specialist service system is an important mechanism
for addressing the relative disadvantage experienced by Australians with
disabilities, the data sets that are collected only indirectly relate to this
disadvantage. They have been explicitly developed according to the immediate
concerns and priorities of the state and territory governments and
administrators. This means that the data collection framework is largely
reactive in nature in the absence of a long term strategic framework connected
to the higher purpose of the vision contained in the preamble.[24]
4.37
The Office of the Public Advocate argued that it was meaningless to talk
about numbers of service users when what is really needed is an outcome based
measure of how successful is the delivery of services. While outcomes are more
difficult to measure, there has been progress in some areas, for example in
relation to support accommodation for people with intellectual disability where
outcome based reporting is achieved by having personal plans for residents.[25]
The Public Advocate concluded that:
The data collection system needs to be realigned so that
measuring outcomes arising from service interventions for individuals with
disabilities is more robust. Progress could also then be connected to
aspirational national benchmarks rather than being limited to the current comparative
benchmarks between jurisdictions.[26]
4.38
The NSW Government commented that if there is an outcomes based CSTDA
then comparative data would be required. However, a broader view of effort and
investment in disability could be taken to consider broader outcome indicators,
such as the number of people who are employed, the number of people who are
participating in various activities and the percentage of families who are able
to stay together. The NSW Government commented that 'maybe there is a debate to
be had about whether we want the CSTDA performance indicators to report only on
the activity covered by the agreement or whether we want to take a broader look
at what is happening for people with a disability and how we measure the
success of that' and concluded:
They are two different directions. Whether they could come
together in an agreement like this I am not sure, but I understand and have
some sympathy with the view that we need to take a broader look at what the
outcomes are rather than just having some accountability for the outputs that
the money is buying within the agreement.[27]
4.39
The Tasmanian Government also raised some concern about the cost of
providing outcome data:
There is also a need to get the balance between providing really
good outcome data and the cost. Everyone agrees that we do need good evaluation
data but we have to balance that against what that is going to cost and whether
that money could be used for other purposes. Keeping it to a minimal set of
outcomes is another important point; we need to ensure that we do not get
swamped by the whole accountability agenda.[28]
4.40
The AIHW indicated that data on outcomes for individuals was to be included
in the existing minimum dataset but was abandoned. AIHW stated that although it
is difficult, there are guidelines in AIHW documentation of how information
about outcomes could be collected consistently. As to why the collection of
this data was abandoned, AIHW commented that practice varies across
jurisdictions, and as improvements on the data sources were about to be
undertaken, to also include this additional information on comparable outcome
information might have seemed a very expensive task and burdensome to data
providers.[29]
4.41
FaCSIA indicated that the there was a need to augment the current input control
and output reporting with an outcomes reporting framework.[30]
This could be undertaken at the service provider level or through a survey. FaCSIA
concluded:
The issue with looking at the collection at the service provider
level...is the difficulty services face already in providing and collecting data.
That is a set of discussions we need to have with the states and territories – and
with the [AIHW], to get their advice on the best way to move forward. But the
minister does think it is important to more clearly measure whether or not the
services we are purchasing are getting the outcomes we expect that they should
get for people.[31]
Conclusion
4.42
The Committee notes the significant improvements that have been made in
the data collection for disability services. However, there are still gaps and
inconsistencies in the datasets. The collection of accurate data and the timely
remittance of that data involve administrative time and costs for service
providers and the Committee welcomes the initiatives undertaken by the State
and Territory Governments to assist service providers to remit accurate data.
4.43
The Committee is also supportive of further research being undertaken on
the datasets which are currently available as this would provide much more
information to assist planning of disability services. As the AIHW pointed out
there is potential for further detailed analysis, however additional funds are
required for this work to be undertaken. The need for data on outcomes was a
major concern raised by witnesses. The Committee also considers that it is a
fundamental flaw in the datasets for disability services to not be able to
identify if the aims of one of the major programs of government are being
achieved.
Recommendation 15
4.44
That additional funding be made available under the next CSTDA to:
- enable further analysis using the CSTDA data collections, to
better inform policy makers and the public about the effectiveness of
disability services; and
- enable jurisdictions and service providers to improve CSTDA NMDS
data.
Recommendation 16
4.45
That the Commonwealth ensure that outcomes data is included in the CSTDA
National Minimum Dataset.
Continuing unmet need
In my experience of people with disabilities who access CSTDA
funds there is a feeling of hopelessness in the sector which is leading to a
great underestimate of the degree of the unmet need and I reiterate that the
national minimum data set really only measures the services delivered and
ignores what is needed.[32]
4.46
As noted above, the AIHW 2001 study identified a high level of unmet
need. While governments have responded to increasing demand for specialist disability
services, witnesses pointed to evidence of a growing gap between demand for
disability services and the supply of those services. That gap is yet to be
identified as the results of the current AIHW have not yet been released.
However, evidence provided to the Committee goes some way to identifying the
magnitude of the unmet need in the service areas covered by the CSTDA.
Accommodation support services
4.47
State and Territory Governments administer accommodation support
services that provide support to people with a disability in accommodation
settings (hostels, institutions and group homes) and the community (attendant
care, personal care and in-home support). In total, 33,787 people received
accommodation support services during 2004-05. More than half (56 per cent) received
community based support to live in the community within their own or family
home. A further 31 per cent were provided with accommodation in group homes and
14 per cent were provided with accommodation in institutions or hostels. Nationally,
4.8 per cent of the estimated potential population were using CSTDA funded
accommodation support services in 2004-05.[33]
4.48
Figure 4.1 shows the use of accommodation support services across
jurisdictions in 2004-05.
Figure 4.1: Service users of accommodation support
services, per 1000 potential population, by service type category, by
State/Territory, 2004-05
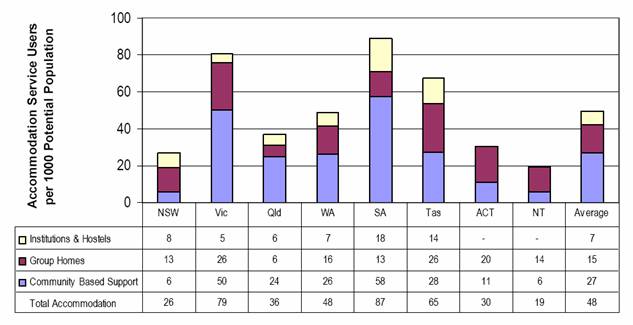
Source: National Disability Administrators, CSTDA Annual
Public Report 2004-05, p.60.
4.49
The average cost to government per accommodation support service user
varies across categories, reflecting the different nature of services. The
national average CSTDA expenditure for the year 2004-05:
- institutions and hostels: $82,389 per service user;
- group homes: $92,949 per service user; and
- community based support: $17,674 per service user.[34]
4.50
Figure 4.2 shows that the majority of accommodation support service
users reported an intellectual disability as the primary disability.
Figure 4.2: Service users of accommodation support
services, by primary disability group, 2004-05
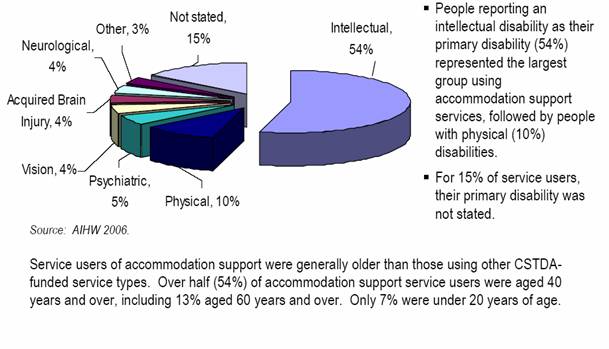
Source: National Disability Administrators, CSTDA Annual
Public Report 2004-05, p.61.
Identification of unmet need for
accommodation services
4.51
While accommodation support services have been identified as the area of
greatest unmet need, the estimation of the level of that need is complex. In
its 2002 report, the AIHW reported that there were 12,500 people needing
accommodation and respite services. However, many witnesses stated that this
did not reveal the true level of unmet need as a number of significant factors
were contributing to the underestimation of the need for accommodation services.
First, many witnesses commented that significant numbers of people with
disabilities whose unmet needs should be addressed by CSTDA funds do not apply
or register for support and services because they know that it is unlikely that
they will ever get into a priority position on a waiting list.[35]
4.52
Secondly, in some jurisdictions waiting lists are not kept so
that there is no way of identifying the level of unmet need or indeed levels of
under-met need. However, evidence was received about some waiting lists which provides
a glimpse of the level of unmet need:
- in Victoria, the waiting list for shared accommodation and
in-home and community support was almost 4,500 people;[36]
- in Victoria, there had been a 76 per cent increase in the number
of people classified as urgent on the waiting list for support accommodation;[37]
- in Victoria, one in six people waiting for supported
accommodation are cared for by family members aged 75 years and over;[38]
- in 2006, the South Australian Intellectual Disability Services
Council had a waiting list for urgent accommodation for 2,200 people with
intellectual disabilities;[39]
- in Western Australia, in relation to Accommodation Support
Funding, unmet demand for 2005-06 was 276 unfunded applicants with a notional cost
to meet unmet demand of $14.9 million.[40]
4.53
Thirdly, some people with disability are not included in unmet
need calculations because they are regarded as being accommodated. However, witnesses
pointed to the many types of unsuitable accommodation that may be used because
essential support services for community integration are insufficient to meet
the needs of people with disabilities. Types of inappropriate environments include
hostels and boarding houses where services are few and people with a disability
are more vulnerable to abuse and exploitation.[41]
People with disabilities living in public housing fare little better:
People with disabilities living in public housing experience
isolation, harassment from neighbours, and often sheer fear of being assaulted
and taunted. Many have no access to any other services, their flats decay, many
feel too embarrassed to ask for help. These are the forgotten, but accommodated
people with intellectual disabilities, for example, or recovering from mental
health problems.[42]
4.54
The Committee also heard evidence of other groups of disabled people who
may be seen as being accommodated but for whom the accommodation did not meet
all their needs. Mr Patrick Eadington, a young person with cerebral palsy, informed
the Committee that he lives in a unit designed for people with disabilities but
he is socially isolated and has no on-going assistance. While there are group
homes available these are mainly for people with intellectual disabilities and
other people who cannot maintain an independent lifestyle, such as people with
a degenerative disease. Mr Eadington stated that his personal preference is to
be accommodated with other people with a similar disability but at the present
time this is not an option even though there are a large number of people who
are in a similar position to himself:
You will find a huge amount of people with physical
disabilities, particularly people who are 30-plus. Because you find the older
they get the more support they need; not that they want support, but they
accept that they need support. You will find a big backlog.[43]
4.55
The Young People in Nursing Homes National Alliance (YPINHNA) noted that
younger people with disabilities living in the aged care system are not
included in the AIHW's analysis of unmet need. However, while they are accommodated
they live in inappropriate settings which do not provide adequate services to
allow them lives of dignity and independence. YPINHNA noted that 70 per
cent of those who receive CSTDA services have an intellectual disability while
over 80 per cent of young people in aged care facilities have an acquired
disability such as ABI, stroke or progressive neurological conditions.
Supported accommodation is very limited for this group with only approximately
1.5 per cent of total expenditure on shared disability supported accommodation
in Victoria being directed specifically for housing services for this group.
YPINHNA went on to state that while it is administratively attractive to absorb
this group into the disability system, 'this cannot be done because the services
required simply do not exist'.[44]
4.56
MS Australia commented that the growth in the number of young people in aged
care facilities 'is a direct expression of the incapacity of the disability
system to absorb additional demand – particularly those people with high and
urgent support needs'.[45]
4.57
Fourthly, the Committee heard evidence of the needs of particular
groups for accommodation services that are not being met currently. WWDA voiced
concerns for women with disabilities who have poor access to housing and are
considered to be of the highest risk for homelessness with data pointing to
lower levels of CSTDA service usage by women. Women with disabilities are also
at great risk of violence and are often forced to live in situations in which
they are vulnerable to violence.[46]
4.58
People aged between 50 and 60 years also appear to have poorly serviced
accommodation needs. Brightwater commented that there were restricted
accommodation options for this group with a disability and that 'it is
questionable whether age should be the main determining factor when assessing
eligibility to participate in Disability accommodation funding rounds'.[47]
4.59
Young people in the acute hospital system with high support needs and
complex care issues are another group which are often poorly identified. Families
receive confusing information from outside agencies about the entitlements of
these young people and which agency has major responsibility for their ultimate
living option. The limited accommodation options that are available to these young
people result in them being placed low on the priority list for disability
funding.[48]
4.60
The Committee also received evidence on the accommodation needs of
people with acquired brain injury (ABI). People with ABI who have high support
needs have few choices in accommodation, due to the limited options. Some will
end up in group homes, while others will be placed in a hostel. Often these
facilities have been designed for a different cohort of people with a
disability, for example people with an intellectual disability or mental
illness. Staff of such facilities are generally unable to respond appropriately
to the complex issues surrounding ABI. As a consequence, people with ABI are
refused access because of the perceived complexity of their support requirements.[49]
4.61
Accommodation services also encompass support for those living at home
or in the community. Evidence to the Committee indicated that these services
are being spread very thinly, with few people accessing the level of services
they require to maintain an independent lifestyle with the quality and dignity
that they wish. MS Australia commented:
We have noticed that the size of available care packages coming
out of disability programs in some states (particularly Victoria) are getting
progressively smaller as the demand on limited growth funds intensifies.
Clearly, as in HACC, it appears that the position has been taken to spread
available resources as thinly as possible over the largest group of people as a
way of managing demand. While this meets the needs of some people, those who
have high needs and progressive conditions have few, if any options.[50]
The Committee heard that the
lack of attendant care services had led some people with disabilities to choose
between having a meal or having a shower.[51]
The Human Face of Unmet Need
T.
suffered brain damage through illness when he was 18 months old and was left
with a severe intellectual disability. He is now 35 years old and lives with
his parents who are 71 and 64 years old.
T.'s parents shower, shave, toilet and dress him each
morning. He cannot go out without having someone with him and cannot be left
alone at home even for 5 minutes. T.'s world revolves around his job with a
local Supported Employment Service which he attends during the week from 9.30am to 3.00pm. He enjoys
listening to music, watching television programmes and travelling on public
transport.
T.'s parents are growing older and realise they will
have difficulty in coping in the near future. T. has been on the waiting list
for Supported Accommodation since 1998 (7 years). In 2001 he moved up to High
priority classification and in 2003 he moved up to Urgent priority.
His parents know that T. will have a long transition
period to his new home and want to be around to help and support him through
what they know will be a difficult period for him.
Source: Submission
33, p.6 (CIDA (Vic))
4.62
Evidence was also provided indicating the difficulties faced by some
groups, particularly those with a degenerative disease, in accessing adequate
services in a timely way. People with a degenerative disability have intensive
specialised care needs over a relatively short period of time: for example,
approximately three years for people with Motor Neurone Disease, five or more
years for people with Multiple Sclerosis. Some people with degenerative
disability remain at home and access support packages. However, the
degenerative nature of their condition means that accurate assessment of
current and future care needs, while crucial, is a real challenge. People with
degenerative conditions must 'line-up' to get access to services.
Client 44 – Is a sole parent of
adolescent boys. Her MS has deteriorated significantly and she immediately
requires assistance with personal care and meal preparation. In attempting to
carry out these tasks she is experiencing falls and extremely high fatigue
levels, which are putting her health and safety at risk. She requires
assistance with showering, dressing/undressing, transfers and is having to rely
increasingly on emergency services due to urinary and bowel accidents. Client
44 currently receives 13.5hrs per week for assistance with personal care and
7.5hrs for household tasks. She requires an additional 1.5 hrs per day with
personal care in the evening, 2 hrs per week assistance with meal preparations
and 2 hrs per week with household management. Client 44 has reported incidences
of verbal abuse from her sons, which she attributes to their inability to come
to terms with her condition and its deterioration. This client is at immediate
risk of family breakdown and institutionalisation if the above supports are not
put in place.
Source:
Submission 88, p.9 (MS Australia of
SA and NT)
4.63
Allowance for professional support is usually not factored into
estimated cost of care, and is often calculated only at a care worker rate.[52]
MS Australia reported that a number of HACC Linkages services in Victoria
refuse to take people with progressive neurological conditions into their
programs because they are expected to have escalating needs that will clog the
program and put stress on their budgets and waiting lists.[53]
4.64
In some jurisdictions age impacts on the amount of in-home services
provided. For example in Victoria, 'Home First' packages which can provide
support up to 34 hours per week are open only to those under the age of 65
years.[54]
4.65
People with ABI are another group with specialist support needs who face
difficulties in obtaining services. They require practical assistance to
complete rehabilitation, develop social networks, obtain employment, and participate
in their communities. Brain Injury Australia commented that given the
complexity and diversity of the services that may be required (an average of
over four different types, according to one recent study), it is unlikely that
a single service provider can meet all the needs of a person with ABI. Brain
Injury Australia supported cohesive, cross program strategies to ensure
appropriate care and support is provided to those with ABI.[55]
Mother in mid 50s, caring for three members
of her family. 15 year old son with severe intellectual and physical
disabilities, needing PEG feeding every three hours, positioning in his
wheelchair, bathing. He is unable to communicate and at night needs changing
and repositioning in his bed. 21 year old son has kidney disease, he has had a
kidney transplant but still needs dialysis three times pre week, and he is
severely depressed and has tried to commit suicide once. Dad is undergoing
treatment for cancer, and is so depressed will not come out of his bedroom.
Mother applied for some in home support to allow her to spend time with he
husband and other son. She was refused funding.
Source:
Submission 66, p.2 (Committed about
Securing Accommodation for People with Disabilities)
Options for accommodation services
4.66
The Western Australian Government argued that the Commonwealth was
failing to assist with unmet need for accommodation services:
The Australian Government has consistently refused to take any
responsibility for funding of accommodation services, even when there are clear
links between their funding priorities and the capacity of the states to meet
the needs of carers and people with a disability.
At the same time the Australian Government demands greater efforts on all
fronts and the States and Territories are left with the dilemma of not being
able to deliver the required level of services in areas that are important in
the long term (such as early intervention) in order to meet basic but critical
needs such as accommodation for people with high support needs.[56]
4.67
The Western Australian Government went on to comment that under the
first CSDA there was agreement that funding and administrative responsibilities
would be shared between both levels of government. It was understood that while
the States had administrative responsibility for accommodation services, the Commonwealth
would continue to make a solid contribution towards meeting the cost of
State-administered services, particularly accommodation. The Government
concluded 'it is of concern that increasingly the Australian Government appears
to see accommodation, with its huge demand factors, as being solely a State
funding responsibility'.[57]
4.68
Western Australia indicated that it had increased disability funding in
2006-07 by 11.7 per cent which would enable more people to receive disability
services, including an additional 113 to receive accommodation support. The
Western Australian Government concluded that 'the shortfall in Australian
Government funding, compounded by Western Australia’s historical low equity
share, means that people with disabilities continue to miss out on much-needed
support, including accommodation'.[58]
4.69
The Victorian Government commented that a commitment is needed from all
levels of Government to pursue options for affordable housing. The Commonwealth
needs to ensure that welfare payments in relation to rent assistance are
sufficient to gain access to housing in the contemporary market as demand for
low cost and affordable housing continues to grow.
4.70
The Victorian Government argued that central to managing unmet need is
the provision of alternative accommodation options. Strategies should include
options beyond traditional models of supported accommodation such as group
homes and require tailored packages of support linked with housing options, the
provision of early intervention and support for carers, and targeted strategies
to promote skills development and participation of people with a disability to
heighten independence. The capacity for group homes to support people with a
disability using a more individualised approach and a greater emphasis on
transition by encouraging more independence in the community needs to be
explored, as do innovative service options.[59]
4.71
However the Commonwealth noted that accommodation is an area of State
and Territory responsibility under the CSTDA. It also noted that 'poor data
provided by the states and territories and delays in establishing new or
expanded services with the additional funds provided to address unmet need, has
meant that it is now difficult to determine whether the additional funding has
effectively addressed the unmet need identified in the 2002 AIHW report'.[60]
In its submission the Commonwealth also highlighted it also provides
contributions to accommodation services through the Commonwealth State Housing Agreement
and the Supported Accommodation Assistance Program. Approximately one quarter
of people accessing these programs had disabilities.[61]
Respite services
Long-term carers find that 'surviving' is a matter of taking
time out for themselves. Part of this may just be taking time for a cuppa
during each day but often longer breaks are needed. Respite care is an
essential part of the overall support that families may need.[62]
4.72
The AIHW has estimated a potential population of 215,511 people who will
require respite services at some time.[63]
Evidence indicates that there are very high levels of unmet need in respite
services. Many carers are unable to access the hours of respite they need and
services are constantly juggling resources to try to meet client requirements.
4.73
Interchange Respite Care identified the main concerns with respite
services as:
- services are difficult to access and the service system landscape
seems to be fragmented and complex;
- availability of respite support is decreasing;
- service support needs to be flexible and responsive to meet
individual needs; and
- many families and carers believe their future respite needs will
only continue to increase.[64]
4.74
The shortage of respite places is exacerbated by other shortages in the
disability sector, particularly long-term supported accommodation. Witnesses
commented that in many respite services bed blocking occurs because there are
no alternative long-term accommodation options available for people with
disabilities. Such practices exacerbate the already desperate situations for
some families who are only seeking some short-term respite but cannot do so
because of the lack of places:
We receive some respite which helps but respite has issues too,
there is simply not enough! The beds are continually blocked and will continue
to be so as more and more families go into crisis. This (respite) is where they
put the children of those families. You must understand that by blocking the
beds, families get less respite and consequently they too may go into crisis.[65]
4.75
The Western Australian Government welcomed the additional funding under
the Older Carers Bilateral Agreement but stated that this agreement 'is
implicit acknowledgment of the continued unmet need in disability services'.
The Government, and other witnesses, argued that additional funds are required
for long-term accommodation support. Respite care is also used to hide need in
other areas including day programs and vacation care programs. Older carers are
in great need and that 'for this group in particular, offering additional
respite gave no sense of security or confidence that their loved one would be
well cared for when they were no longer able to do so themselves'.[66]
4.76
Interchange Respite Care commented that 'respite has been seen and used
by governments and bureaucrats as bandaid solutions and forced some families
into situations of permanent care roles which they ultimately do not wish to
pursue'.[67]
A witness provided the following case:
I have a friend who developed breast cancer; she is a sole parent
Carer. When she was hospitalised for surgery, her mother was supposed to care
for her 16 year old son. Her mother, wise to the ways of government, unbeknown
to my friend, sent her son off to respite care, saying she could not cope. When
my friend came home from hospital, she was too sick to bring him home. She came
to realise, with the support of her mother, that her son was happy and that
this was her opportunity – it might never come again, so she decided to refuse
to bring him home. He stayed in respite care for 8 months, finally the
government realised she could not be manipulated into taking him back and found
him a permanent placement.[68]
4.77
The Committee also heard evidence about the lack of respite options for
people with specific disabilities such as ABI. The Brain Injury Association of
Tasmania commented that there is a significant and pressing need for respite
models which are affordable, age appropriate and are staffed with support
workers that are educated regarding the needs and best practice service
delivery models for people with ABI. These respite services should be available
in a community based and/or home based setting and should focus on offering
flexible, needs based services which are part of a planned, individualised
support program.[69]
4.78
For people with degenerative conditions such as MS, respite is often
limited to time in an aged care facility. Young people are generally reluctant
to take up these options, don't enjoy the experience if they do go and
facilities find it difficult to provide the type of care they need.[70]
Hopes Inc noted that often facilities only have one respite bed and this may be
in a dementia unit: 'to be totally surrounded by people with varying stages of
dementia and to be physically unable to move out of the locked unit, is
incredibly stressful for a younger person used to family support in their own
home'.[71]
4.79
The overwhelming evidence received by the Committee indicates that the
provision of adequate respite care is fundamental to enabling people with
disabilities to continue to be cared for within families. Significant levels of
unmet need for respite services were identified with the result that many
families are unable access adequate respite unless they face a crisis
situation. In part, the lack of respite services is due to problems in the
provision of other services most notably accommodation services. Witnesses
pointed to reduced access to respite facilities arising from the lack of
accommodation options for people with disabilities whose families are no longer
able to care for them. This, in turn, decreases the number of respite beds
available and so places greater pressure on families seeking short-term respite
options.
Assistive technology
4.80
Assistive technology (aids and equipment) is not included in the CSTDA.
However, its importance to people with a disability cannot be underestimated:
assistive technology can provide individuals with greater personal
independence; improve quality of life; assist with social inclusion; and reduce
the demand for costly personal assistance. Investment in aids and equipment assist
people to remain at home thereby diverting from more costly disability or aged
care support options. Aids and equipment can reduce the need for out of home
placements through avoiding hospital admissions (for example because of
pressure sores from poor equipment) and can enhance the longer-term capacity of
carers (for example the use of hoists). YPINH National Alliance commented that
delays in accessing much needed equipment leads to diminution of health and
independence and a consequent increase in the health and support costs borne by
government. It is a false economy when Australians with disability cannot
access the equipment they need.[72]
Client M4 is a single man aged 42
years living alone in cluster style accommodation. This Client describes his
living experience as being 'solitary confinement'. The client reports carer
attendance to his needs morning and evening and his mother helping with his
meal in the middle of the day. Client says he spends his day watching TV as he
cannot independently get around his home and cannot access his computer/music
etc independently. This is due to the client no longer being able to manage a
manual wheelchair. Client asks that he be allocated an electric wheelchair as
this will allow him to move around his flat. He indicated he had been on the
waiting list for this equipment for at least 18 months. The client says he does
not see anyone else day after day and does not have the opportunity for any
meaningful activity. He has little or no contact with the young people in the
other flats that make up the complex of 7 units.
Source: Submission 88, p.10 (MS
Australia of SA & NT).
4.81
The AIHW reported that some research suggests that aids and equipment
alone may be a more efficacious form of assistance than personal assistance in
reducing difficulty associated with performing tasks of daily living.[73]
Nearly half of all people with disabilities use assistive technology but there
continues to be high unmet need.
4.82
Both the Commonwealth (through the Departments of Health and Ageing,
Veterans' Affairs and Employment and Workplace Relations) and the State and
Territory Governments administer schemes which provide cost-free or low-cost
aids and equipment to people with disabilities. A range of non-government organisations
and health insurance organisations also provide access to assistive equipment.
4.83
Access to assistive technology varies with the provider and across
jurisdictions. The Independent Living Centre WA commented that the criteria for
funding eligibility vary from State to State which leads to confusion and inequity:
What you find when you start to look into it is that each state
has totally different, separate, individual programs that they are running that
are state funded. We have great variation in access to funding from state to
state. The amount of funding – the ratio per capita – varies from state to
state...[74]
4.84
In addition, narrow definitions of assistive technology in all States
serve to restrict access to those most in need. There are multiple barriers to
embracing assistive technology in addition to the funding and policy obstacles.
These include the volume of change facing organisations, lack of consumer
pressure, organisational fragmentation and technology phobia present amongst
many members of the disability sector.[75]
4.85
Current schemes fall short in meeting demand and timely provision of
appropriate equipment. Waiting times for equipment can be long. MS Australia
commented that there are people with MS who have experienced long periods of
hospitalisation for skin breakdown (pressure sores) because their equipment
needs could not be met. In many situations the prescribed pressure mattress or
wheelchair could not be fully funded through the Government schemes, and the
additional resources could not be secured, so the person has tried to get by with
inadequate or no equipment.
4.86
Funding limits for equipment like mattresses or wheelchairs can be as
little as 50 per cent of the purchase price, leaving the individual and the
family to find the difference. In most cases the $4,000-6,000 required is
simply not there. This is also a common reason for young people being admitted
to nursing homes, because either their disability is worsened by the lack of
correct equipment, or the effort required by families to care for a person with
a severe disability without the right equipment is overwhelming.[76]
4.87
Other schemes are fragmented by Commonwealth-State divisions and
under-supply. MS Australia noted that there are 40 separate equipment programs
in Australia, which is overwhelming. State and Territory Governments, Workers
Compensation and CTP schemes, hospitals, aged care providers, HACC, disability
brokerage programs, Veterans' Affairs, the Workplace Modifications Scheme and
School Education integration programs all are discrete purchasers of equipment.
An example is the Continence Aids Assistance Scheme, which the Federal
Department of Health and Ageing funds for people 16 to 65 years but not for
people over 65 years unless they are in paid employment.[77]
Once a person turns 65 they are no longer eligible for this program and must
find an alternative source of support. MS Australia commented 'this is one area
of split responsibilities that is difficult to defend from any standpoint'.[78]
...one patient with a permanent
tracheostomy was declined DVA funding for suction equipment and was then denied
home modifications to make way for his existing equipment because he has a DVA
card. Most alternative public funding options will exclude access to those
holding DVA cards, hence this patient had no alternative funding source.
Source:
Submission 70, p.4 (APA).
4.88
In its 2003 study of aids and equipment AIHW found there to be 'a
limited range of equipment, problems with cost, availability and shortage of
referral services in remote areas of Australia, and a decline in equipment
supply from traditional dispensing units such as hospitals. Systems for the
provision of equipment appear to be nationally fragmented.'
4.89
Other reports reinforce the AIHW's findings: a 2002 NSW report into the equipment
needs of children found that the processes of equipment provision are slow and
inefficient and that children do without prescribed items for long periods.
Because of the high costs associated with some equipment, families often need
to seek external support to purchase items.[79]
4.90
In 2006, the AIHW published a review of therapy and equipment needs of
people with cerebral palsy and like disabilities.[80]
The AIHW reported significant levels of unmet need, with long waiting times
particularly for those living in non-metropolitan or lower socioeconomic areas
and for adults. Equipment schemes were fragmented and complex with excess
paperwork, restrictive conditions of use and supply adding to inefficiencies. The
AIHW provided some examples of waiting times for equipment for people with
cerebral palsy:
- in Western Australia, the cost of equipment on the Community Aids
and Equipment program in June 2006 was $255,000;
- in May 2006, The Spastic Centre was waiting for funding for 378
equipment items; and
- in August 2006, there were 241 outstanding requests for funding
from the Independent Living Equipment Program made by clients of the Novita
Children's Services South Australia worth about $661,000 in total.[81]
4.91
The AIHW estimated that the annual national cost of meeting unmet need for
equipment for people with cerebral palsy and like disabilities ranged from
$3.5 million to $4.4 million.[82]
4.92
People with a disability also face problems of retaining specialised
equipment and accessing new equipment if they move between States. Mr Ben Lawson
gave this example:
...my powered wheelchair is provided by Queensland Health through
a scheme called 'Medical Aids Subsidy Scheme' (MASS). My wheelchair with its
specialised modifications is worth approximately $10 000. However, if I
were to move to another Australian State I would have to hand back the chair
and its modifications to Queensland Health. Apart from the obvious question of
what I would do without a wheelchair in the interim, I would then reapply in
that state and hope that my application was considered speedily.[83]
4.93
Access problems also arise when people with disabilities move into the
aged care sector. The Motor Neurone Disease Association of Australia noted that
while residential aged care facilities are required to provide appropriate aids
and equipment, most residential services do not have the funds to provide
equipment that is necessary for people living with motor neurone disease. This
is also the case for other groups of people with a disability living in aged
care such as those with acquired brain injury and multiple sclerosis.[84]
Access to specialised equipment is further diminished in some jurisdictions as
State government aids and equipment programs specifically exclude people living
in aged care facilities. In addition, aged care facilities only provide basic
care which does not address the aspirations of young people with a degenerative
disability.[85]
4.94
The Victorian Government noted that there are a range of factors influencing
demand for aids and equipment, including population ageing. Moves to support
more people with a disability or people who are ageing at home or in the
community also have an impact on demand. A heightened awareness of health and
safety issues has led to increased requests for expensive equipment such as
hoists and beds.
4.95
The impact of changing technology and increasing costs is making the
purchase of aids and equipment prohibitive to many people with a disability and
their families due to affordability. The Victorian Government suggested that the
Commonwealth should consider offering financial assistance by way of tax relief
to people with a disability and their families to assist with the affordability
of some aids, equipment and essential home modifications. Such a move would
recognise the high costs incurred by people with a disability due to their
impairment.[86]
4.96
MS Australia also commented that the CSTDA signatories are major purchases
of equipment but there is no mechanism across programs (and in some cases
within programs) to improve purchasing power and to improve pricing. MS
Australia went on to state that this lack of attention to purchasing also means
that there is little or no expectation of service level agreements with
suppliers or customers.
4.97
MS Australia pointed to the system used by the Department of Veterans' Affairs
as a model that goes close to what is required in disability services. The
Department's equipment brokers delivery good price and service outcomes through
purchasing agreements and referral processes.[87]
The
Victorian Aids and Equipment Program (VAEP) is a Victorian Government program
which aims to assist children and adults to access subsidised aids, equipment
and home modifications to enhance their safety and independence, support their
family and carers and prevent premature admission to institutional care or high
cost services.
Unfortunately, if a client lives in any sort of
supported accommodation (ie a Residential Aged Care Facility) they are not
eligible for equipment through VAEP and supported accommodation funding does
not cover equipment purchase.
Patients being discharged from hospital to nursing
homes are not eligible for equipment. I have had two patients recently in their
50's and needing high level care who need motorised wheel chairs or custom made
chairs to re-enter the community. Both patients have the family and community
support necessary to re-enter the community but they can’t do so because of
lack of equipment. If they lived in the community they would be eligible for
equipment.
Source: Submission
70, p.4 (APA).
4.98
There was widespread support for the development of a national strategy
for the provision of aids and equipment. The Independent Living Centre
commented:
A national approach to access, support, and funding of AT is a
vital step to inclusion and participation across Australia and an essential
response to the rapid the rate of growth and change occurring in AT. It is
important to the future of Australians with a disability, and those yet to have
a disability, that AT be included in the next CSTDA.
AT is a vital component in the development of a national policy
and service framework. The correct coordination, disbursement and application
of AT is an economically sound strategy which can enrich the quality of life of
people with a disability, meaning more people return to work, live safely in
their own homes and actively participate in their community. In the current
climate of workforce shortages AT has a significant role to play, reducing the
volume of personal care services required by those with a disability and the
frail aged and keeping people in the workforce.[88]
4.99
Witnesses pointed to the work undertaken by Ernst and Young on equipment
needs for the 1996 evaluation of the Commonwealth State Disability Agreement.
It was recommended that a National Equipment Strategy be developed to improve
the range and timeliness of equipment provision and lower the cost of
maintenance and repairs. The evaluation report recommended that work be done
around equipment services so that it is strategically integrated with the rest
of the specialist disability services system, its is accessible to all people
with disabilities who need equipment and is provided for in ways which are
customised appropriately.[89]
4.100
The evaluation report stated that just bringing equipment into the CSTDA
is not enough:
What this would mean in any case cannot be resolved without
giving attention to the policy issue of just what is and should be the
strategic role and place of cost effective equipment services within an
integrated disability service system. It is important to emphasise that 'it is
a policy issue in the first place, not a program management one, as it has been
taken to be'.
4.101
ACROD concluded that the need for such a strategy is now pressing with the
CSTDA providing an appropriate multi-lateral framework under which to
coordinate such a strategy.[90]
4.102
The Australian Physiotherapists Association (APA) argued that a national
strategy should include:
- responsive and timely provision of aids and equipment for all
people with disabilities that meet both their short and long term needs;
- strategies to build national purchasing power in the equipment
market, while retaining local individualised clinical assessment and provision;
- more inclusive and nationally consistent eligibility criteria;
- an end to arbitrary access barriers such as age; and
- equitable access for people waiting for, and accommodated in,
residential aged care facilities; people living in rural and remote areas;
people with hearing and/or visual impairment; and for Indigenous Australians.[91]
Recommendation 17
4.103
That the Commonwealth, State and Territory governments implement a national
equipment strategy as part of the next CSTDA.
Early intervention
4.104
Witnesses commented on the importance of early intervention. ACROD
stated that early intervention means both providing assistance before a problem
escalates into a crisis and providing support and therapy early in life to
enable a child or young person to develop well and fulfil their potential.[92]
4.105
Early intervention assists children and young people to grow, learn and
achieve, and it can prevent the development of secondary disabilities. All
family members benefit from the improvements in the life of the child or young
person. However, concerns were raised that many children and young people with
disability lack adequate access to programs that would encourage their optimum
development.
4.106
Mr Bob Buckley raised the particular needs for early intervention for
young children with autism. Early diagnosis and specialised early intervention
are proven methods for minimising the level of disability children with autism
spectrum disorder carry into adulthood. However, there are waiting lists of up
to two years for diagnosis in the public system while private assessment cost
about $1,500.[93]
4.107
Research points to the need for a minimum of 20 hours per week of
effective early intervention for children with autism. However, Mr Buckley
noted that 'in Australia there are no government-funded programs providing the
recommended amounts of intervention'. Mr Buckley also pointed to shortcomings
in the services governments and their agents provide as they do not offer an
appropriate level of language and communication intervention, social skills
development and skill development in other key areas. The programs also lack
appropriate professional supervision and monitoring of program outcomes. These
programs are not evidence-based; in fact they are programs of a type that is
known to be inappropriate and ineffective for children with autism. Mr Buckley
concluded:
The existing process leaves many parents without appropriate
information. And it denies equality of opportunity to many children who are
severely disabled by their autism. It means they do not have the opportunity to
develop skills that are critical to their success in education, and
subsequently in employment and community participation.[94]
Recommendation 18
4.108
That the next CSTDA include a commitment of additional funding for early
intervention.
Employment services
4.109
The 2002 AIHW report on unmet need estimated 5,400 people needing
employment support.[95]
In 2000-01, a total of 60,352 people with disability accessed specialist
employment services while in 2004-05, a total of 68,370 people with disability
accessed these services – an overall increase of 8,018 or 13.3 per cent. Over
this time period, funding for specialist employment services increased from
$241 million to $352 million.[96]
4.110
The Commonwealth commented that in considering unmet need for specialist
disability employment services, it should be noted that service capability is
just as important as the number of places available. The Commonwealth's reforms
to specialist disability employment services 'have had a small but observable
impact in broadening the focus of specialist employment services from a
traditional focus on intellectual disability to supporting people with a much
wider range of disabilities'. For example, service users with autism increased
from 1.7 per cent in 2001-02 to 2.3 per cent in 2004-05 in open employment
services and over the same period the proportion of service users with specific
learning difficulties and attention deficit disorder rose from 9.2 per cent to
10.3 per cent. Supported employment services have shown similar increases.
4.111
People with intellectual disabilities are increasingly choosing open
employment over supported employment services. In 2004-05, there were 12,325
people with intellectual disabilities using open employment services (26.8 per
cent of all clients) and 14,097 service users with intellectual disabilities
accessing supported employment services (73.4 per cent of all supported
employment clients). This is significant change since 1997 when people with
intellectual disability made up 48.3 per cent of open employment users and 77.9
per cent of supported employment clients.
4.112
The Commonwealth commented that the introduction of individualised, case
based funding for supported employment has resulted in a marked shift towards a
client group with much higher support needs. In the three years from 2002 (the
year before case based funding places began to be released) to 2004, supported
employment service users were increasingly likely to have a profound core
activity restriction. Over that period:
- the number of supported employment clients with a profound core
activity restriction increased by 28.6 per cent nationally;
- the number of supported employment clients with a severe core
activity restriction increased by 15.3 per cent nationally; and
- the number of supported employment clients with a core activity
restriction of 'moderate to none' has fallen by 13 per cent nationally.
4.113
Additional evidence that case based funding has been effective in
directing supported employment services increasingly towards those with higher
support needs can be found in data from the annual Disability Services Census. Those
data show that the proportion of supported employment clients who receive care
has increased from 66.4 per cent in 2002 to 73.7 per cent in 2004.
4.114
The Commonwealth concluded that the ongoing commitment of the Government
to improving employment outcomes for people with disability is demonstrated in
the 2005-06 Budget announcement of an additional 21,000 demand driven
(uncapped) places in the Disability Employment Network, which have become
available since July 2006.[97]
4.115
The Western Australian Government did not support the view that Commonwealth
employment programs showed a shift towards clients with higher support needs. The
Western Australian Government pointed to the following data to support its
claims:
- direct staff hours have remained constant while the number of
people accessing the program has increased by 30 per cent;
- indirect staff hours have fallen by 14 per cent;
- there has been a major change in the proportion of people with intellectual
disabilities from 62 per cent in 1998 down to 41 per cent in 2004;
- there has been a significant increase in the proportion of people
with low support needs from 11.5 per cent in 1998 to 23.5 per cent in 2004;
-
in the period 1998-2004 there has also been a significant change
in the number of hours people with disabilities are working, with more program
participants working less than two days per week;
- the proportion of Western Australians with a disability employed
for 15 hours or less has increased from 18 per cent to 29 per cent; and
- the proportion of Western Australians with a disability employed
for 30 hours or more each week fell from 53 per cent to 43 per cent.[98]
4.116
The Western Australian Government commented that the introduction of the
Commonwealth Disability Services Act 1986 had been the impetus for
stringent Commonwealth driven reforms to employment support for people with
disabilities. In addition, since 1997 the Commonwealth reforms have 'significantly
redefined the scope of the Disability Employment Program, that is, who is
eligible, and what is considered to be an employment outcome'. States andTerritories
were not consulted about this process and 'represents a fundamental shift in
the interpretation of responsibilities on which the first Commonwealth/State
Disability Agreement was negotiated'.
4.117
MS Australia also commented on the introduction of very strict rules of
eligibility, type of service and financial incentives for providers when the
Disability Open Employment Program moved to DEWR in 2005. MS Australia stated
that 'while we would support the increased opportunities to work, much of the
system is out of step with the other aims of the CSTDA of individualised
service, linking to other sectors and choice'.[99]
4.118
The Western Australian Government also noted that at the same time these
changes were being implemented, sheltered workshops were redefined as 'Business
Services' and required to adopt a 'duality of focus', such that they would
continue to be a human service provider, but were required to operate
commercially viable businesses. As a consequence, 'people with low productivity
were sacked from services and new people sought to fill vacancies had to be
productive'.[100]
4.119
The Western Australian Government concluded that it continued to be
concerned about the impact of changes and reforms to the Commonwealth
employment program, including:
- reduced access to assistance for people with high support needs,
with particular concern expressed about school leavers;
- increased care responsibilities/pressure on families; and
- the cost-shifting implications for States and Territories.[101]
4.120
The Western Australian Government also commented that progress in the
employment area has been hampered by changes to Commonwealth administrative
arrangements whereby business services remain under FaCSIA and job network
services (formerly known as open employment services) moved to DEWR. This has
added an additional layer of complexity to communications and, as with aged
care, DEWR was required to take on work plan commitments from the general
bilateral agreement.[102]
4.121
Other areas of concern included the transition of people with a
disability from school to work and the impact of the Welfare to Work reforms. The
Western Australian Government commented that the jointly funded Post School
Options (PSO) programs were one way for school leavers with high support needs
to succeed in a range of individually supported jobs and in open employment.
With these other options available to them, very few school leavers chose
sheltered workshops. However, the introduction of Centrelink has impacted on the
Western Australian PSO program and program demarcations 'once again became
barriers, particularly for school leavers with high support needs'.
4.122
The Victorian Government supported greater coordination of programs to
improve the employment options for school leavers:
...there are opportunities for the Commonwealth and the state to
work together in a more coordinated way to increase employment opportunities
for school leavers. The state operates a post-school planning and transition
program for school leavers. The Commonwealth operates employment services and,
whilst there is cooperation now, an agreed strategy with clear outcome targets
could be developed between the jurisdictions to achieve higher workforce
participation for school leavers.[103]
4.123
Jobsupport Inc (an open employment service) also commented that the
current CSTDA interface arrangements between Commonwealth funded Disability
Employment Network services and State funded Post School Options services are
an obstacle preventing people with a significant intellectual disability who
want to work from working. Commonwealth funded capped Disability Employment
Network places are not always available because the program is capped. Post
School Options service users and their families don't want to be without any service
and some are reluctant to attempt open employment because it can be difficult
to re-enter Post School Options if the open employment attempt is unsuccessful.
4.124
Jobsupport noted the significant savings to government of increased
workforce participation by people with disability. Research by Econtech
demonstrated that if approximately 8 per cent (just over 2,000) of the Post
School Options users across Australia moved from Post Schools Options to Open
Employment recurrent budget savings of $21 million would be made. Jobsupport
concluded that:
We simply want to highlight the fact that an opportunity exists
to let people in State Post School Options services who want to work do so,
while at the same time saving the taxpayer money. All that is needed is a more
flexible interface between the Commonwealth and State Governments including the
removal of the cap on Capped Disability Employment Network services.[104]
4.125
Many witnesses raised concerns about the impact of the Welfare to Work
changes introduced by the Commonwealth in 2005.[105]
4.126
MS Australia noted that Welfare to Work is designed to achieve increased
employment outcomes for those who are not working, and has not considered the
impact on this system on those who are, but who need support. It has mostly
ignored the need for job retention services, and is almost totally geared for
finding new jobs for people who are not working at all. In fact there are
exclusions to Disability Employment Services being able to work with those
clients who are working – so the opportunity for a person in this risk group to
seek job retention support is close to zero.[106]
4.127
Women with Disabilities Australia placed particular emphasis on the
needs of disabled women in gaining employment. WWDA commented that 'with one of
the lowest rates of labour force success and one of the highest rates of
poverty, women with disabilities clearly stand out as a group in need of
greater opportunities for employment'. However, little assistance has been
provided to women. Commonwealth funded open employment services assisted over
35,000 people with disabilities to find employment and maintain jobs but 65 per
cent of those assisted were men. Only 9 per cent of women with disabilities are
in full-time employment compared to 21 per cent of men with disabilities. More
women with disabilities are employed part-time (11 per cent) than men (6 per
cent) and 'in any type of employment women with disabilities are already more
likely to be in low paid, part time, short term casual jobs'. WWDA concluded
that 'it is clear that the CSTDA has had little effect on the situation of
women with disabilities in relation to employment'.[107]
4.128
The NCID commented that the Commonwealth does not provide employment
support to all people with intellectual disability who want to work which forces
many people with intellectual disability onto State/Territory funded
alternatives to employment services or to be at home with parents. However, people
with a significant intellectual disability can obtain and keep a job which
benefits not only the person with an intellectual disability but their families
as well. The NCID considered that the major obstacles are a lack of commitment
from the Commonwealth to provide flexible funding and uncapped funding.
4.129
NCID noted that for job seekers with disability who are not seen to be
able to work at award wages for more than 15 hours per week (without support)
funding is capped to a limited number of 'places'. The consequence of this is
that some State and Territory Governments have begun to provide pre-employment
and employment support to job seekers with a disability, funding which the
Commonwealth should be picking up while the States and Territories fund alternatives
to employment programs.
4.130
NCID concluded that job seekers with disability need flexible funding
that can be used to gain pre-employment skills and to engage the employment
support provider of their choice. For example, at the moment there are
significant vacancies within the supported employment network, and given that
employment support is now provided on a case based model, school leavers should
be offered not a place in a service but the funding to approach a service
provider of their choice. There is a clear need for Governments to provide
funding (with clear assessment and accountability criteria) and not to be
involved in choosing service models for people with disability.[108]
Recommendation 19
4.131
That the Commonwealth increase the number of places in the Disability
Employment Network for people on the Disability Support Pension who do not have
mutual obligation requirements.
Transport
4.132
The problems that people with disability face in accessing transport
were raised in evidence. Not only is there a shortage of suitable transport,
the cost of accessing that transport is often prohibitive. This is particularly
the case for people with disability living in rural areas. Brain Injury
Association of Tasmania provided the Committee with a glimpse of the
difficulties of accessing suitable transport for people with a disability in
rural areas:
[In] Launceston, Burnie, Hobart there are some wheelchair
accessible taxis, but this is an expensive service, often limited by
availability. For others, there are few or no accessible transport services in
their local community. This results in an inability (or at least, a reduction)
in the person's capacity to participate in therapeutic services, and ultimately
contributes to social isolation.[109]
4.133
Those people who live in areas where air travel is the only means of
accessing necessary rehabilitation and support face additional financial
burdens. BIA of Tasmania also commented that people with ABI have expressed
feeling vulnerable when accessing public transport. Often taxi drivers do not know
how to safely secure wheelchairs into vehicles and people with ABI experience
difficulties in reading and interpreting public bus timetables.
4.134
ACROD emphasised the importance of transport not only to improving the
social inclusion of people with disability but also to their ability to
participate in the workforce. ACROD argued that as the ability to get to work is
crucial to workforce participation, the Commonwealth's Welfare to Work Reform
will rest on accessibility of transport. ACROD stated that 'the Australian Government
could recognise that, and engage state governments and realise that getting
people into sustainable jobs also required getting accessible transport, good
access to education and training, proper health management and proper in-home
support—many of which are state responsibilities—then perhaps there could be a
more cooperative approach'.[110]
4.135
Many witnesses noted that the CSTDA does not cover transport issues.
AFDO stated that exclusion of transport 'restricts the relevance and power of
the CSTDA as a strategic planning document'.[111]
FaCSIA commented that there are connections to a range of service systems
beyond those that are covered in the current CSTDA agreement. The rationale for
the set of services that are covered in the current agreement 'stems from its
historical origin, which was to relate it to a transfer of a particular set of
services...it is a question of whether or not that remains a sensible set of
services to cover under the agreement'.[112]
Recommendation 20
4.136
That the importance of access to appropriate transport and Patient
Assisted Travel Schemes for people with disabilities be reflected in the terms
of the next CSTDA.
Continuing pressures on demand for services
4.137
Witnesses also identified a number of issues which are now, or will be in
the near future, placing increased pressure on the need for accommodation
services. Of most significance is the number of older people with a disability
still living at home with ageing carers. Many witnesses pointed to the growing
need to provide suitable accommodation for people with disability in the care
of ageing carers. The Gippsland Carers Association noted that in Victoria there
were some 13,900 people aged over 30 years living with a parent as a primary
carer and 55,600 people nation wide.[113]
The National Council on Intellectual Disability also pointed to the over 5,000
people with severe and profound disability living with parents who are aged
over 65 years as evidence of the level of unmet need.[114]
The AIHW indicated that 6,472 carers aged over 65 years were caring for
CSTDA-funded service users in 2003-04.[115]
4.138
As carer parents age, it becomes a constant concern about what will
happen to their disabled children. The Client Guardian Forum noted that often
children with a disability remain in the family home even though the parent/s
can no longer support their adult children. This leads to a fall in the quality
of life for both the person with a disability and the parents. They remain at
home until a crisis point is reached or the parents die.[116]
4.139
At the same time, more people with a disability are living longer,
particularly those with an intellectual disability. Dr Jennifer Torr indicated
that healthy older people with a disability are being placed into nursing homes
when their family carers can no longer care for them, irrespective of whether
they have an aged related disorder or not:
It is not an uncommon scenario for older people with ID to seek
services for the first time when their ageing parents can no longer provide
care through their own ageing, illness or death. Anecdotally this seems to be a
particular problem in rural areas where people with ID have been supported by
family and community rather than specific CSTDA services.[117]
4.140
The Victorian Government also noted that the impact of technological
advances and increased medical survival rates, particularly in the areas of
premature births and traumatic incidents, has led to increased demand for
support from people who have complex medical and disability-related support
needs. Disability Services in Victoria is increasingly required to provide
appropriate support responses for people with acquired brain injury, spinal
injury and neurological conditions who would otherwise remain in acute health
beds or nursing home placements without adequate interventions.[118]
4.141
It was argued that there was a need for increased supported
accommodation options in order to relieve the stress and burden on aged, frail
and ill carers.[119]
4.142
The incidence of some diseases is also growing: MS Australia reported
that the incidence of MS is expected to grow by 7 per cent over the next five
years.[120]
Conclusion
4.143
The Committee was acutely aware during this inquiry that evidence of
sub-optimal organisation and provision of disability services underscores an
immense personal, social and economic burden affecting hundreds of thousands of
Australians. Although enormous improvements in services levels in the last few
decades can be measured, it is difficult not to be aware that there remain
substantial disparities between the outcomes and living standards of disabled
Australians, even allowing for their disability, and those of others in this
country. The fact is inescapable that physical or intellectual disability today
equates almost ineluctably with lesser opportunities, services, social
inclusion and quality of life that the rest of the community takes for granted.
4.144
The evidence of carers, who undertake so much of the caring, brought
home this reality to the Committee. Many cases were cited of families and loved
ones shouldering enormous responsibilities over decades caring for a person
with a disability, with government or community assistance relieving that
burden only slightly or not at all. The Committee acknowledges that families
will always have a substantial responsibility towards the care of their
disabled members, and that it may never be either desirable or economically
feasible to shift that responsibility onto the community as a whole. At the
same time, the Committee recognises that the weight of that responsibility on
countless families is a crushing and unreasonable one, and that much greater
community assistance in that task is urgently called for.
4.145
This report contains several recommendations for improvements in the
coordination and delivery of disability services. The Committee warmly
recommends that Commonwealth, State and Territory governments embrace these
changes; however, the stark reality is that such change cannot adequately
address the very substantial need within our community. Only large and
sustained increases in resourcing to programmes and services will do this.
4.146
The disability system in Australia is replete with examples of
inflexible access criteria, silo-ed services, bureaucratic application and
assessment processes, poor linkages with companion services and obscured entry
points to programs. It is tempting to view these phenomena as coping mechanisms
for a system which simply doesn’t have enough resources to satisfy the demands
placed on it. The consequent rationing of services throws an added burden on
carers: that of expending precious time and energy chasing help that simply
won’t be there.
4.147
While the Committee has recommended that the responsibility for funding
specialist disability services other than employment should primarily rest with
the State and Territory governments under the CSTDA, both levels of government
continue to have an obligation to provide services that address unmet need.
4.148
How large an increase is required to fully satisfy need is impossible to
quantify at this time. The National Carers Coalition estimated that $10.9
billion was required annually to properly provide accommodation choices to
disabled Australians;[121]
however, other witnesses were unable to place a figure on the cost.
4.149
However, the following comments from MS Australia sum up many issues
associated with unmet need and responsibilities of addressing them:
The first point is to try to measure [unmet need] a lot more
deeply, and that may also lead to a more intelligent agreement, because at the
moment...both jurisdictions blame each other for not doing enough...The amount of
money that is needed to meet that demand at the fullest extent is exponential,
but we do not know whether we need to go to the fullest extent...there are a lot
of families who want to keep caring, so it is much more about looking at
sharing the care between governments, families and communities. It is not just
that it is a transfer of responsibility from families to government, but it is
going to be like that. If it keeps being ignored, people are going to say:
'I've done my share. I've had enough. I'm out of here.' Whereas, if there is a
more measured response early, people will stay in longer.[122]
Recommendation 21
4.150
That Commonwealth, State and Territory governments jointly commit as
part of the fourth CSTDA to substantial additional funding to address
identified unmet need for specialist disability services, particularly for
accommodation services and support.
Navigation: Previous Page | Contents | Next Page