Chapter 4
Issues raised during the inquiry
4.1
The majority of evidence presented to the Committee expressed support
for the excise increase on spirit-based RTD beverages. In addition, the issue
most raised with the Committee was whether the measure goes far enough. It was
suggested that other measures would also be of benefit in addressing the issue of
risky and high risk drinking by young people as part of a comprehensive approach.
There were also a number of questions and concerns about unintended consequences
presented which will be detailed below.
Towards a comprehensive approach
4.2
While supporting the measure as a first step, the majority of submissions
argued that raising alcohol taxes needed to be part of a comprehensive approach
to address the harmful and hazardous use of alcohol which included controlling
supply as well as reducing demand. The only people who did not support the
measure and argued it was a retrograde step were from the industry.
4.3
The National Drug and Research Institute (NDRI), while recognising the
potential of the increase in the excise on RTD alcoholic beverages, drew the Committee's
attention to the body of evidence that showed a package of measures are
required to address the issue most effectively.[1]
This was supported by the Australian Medical Association (AMA) which believed
that a stronger and multi-faceted approach is required to change harmful
drinking patterns which included the use of price signals to discourage alcohol
consumption.[2]
4.4
The Curtin Centre for Behavioural Research in Cancer Control noted that
reviews of international literature indicated that a combination of policy,
economic, educational and environmental measures was required to obtain maximum
results.[3]
4.5
The Royal Australasian College of Physicians (RACP), which supported the
measure as the most cost-effective, cited evidence which found that:
Modelling health-related reforms to taxation of alcoholic
beverages has demonstrated that alcohol tax reform on its own is not effective
and must be carried out in conjunction with other strategies.[4]
4.6
The Alcohol Education and Rehabilitation (AER) Foundation believed that
a holistic solution was required to address excessive alcohol consumption and
that it should not be limited to young people.[5]
The need to address other age groups was supported by the Victorian Alcohol
and Drug Association which also highlighted the need to acknowledge the
cultural context of alcohol use in strategy development:
Strategies to address excessive and harmful alcohol consumption
by young people need to acknowledge the role alcohol plays in young people's
lives as they transition from youth to adulthood. Equally important, strategies
need to address broader cultural attitudes to alcohol and set about effecting
change in attitudes and behaviours across age groups.[6]
4.7
Dr Raymond Seidler, a specialist in addiction medicine, suggested that a
comprehensive national strategy should also address the underlying issues of
alcohol dependence in Australia generally and for young people in particular.[7]
This approach was supported by the AMA which noted the harmful consumption of
alcohol has become part of the culture and this must be addressed. To do so
they advocated a strategy that addressed social norms in the same way as the
efforts to reduce smoking have produced new social norms.[8]
4.8
Submissions noted that all the players involved in the alcohol
issue should be part of the strategy and they encouraged industry to play a key
role.[9]
Submissions from industry pointed out that risky and high risk drinking is an
industry wide issue which requires an industry wide solution.[10]
The Committee notes that evidence from industry representatives
indicated a willingness to be part of a process to produce a comprehensive strategy.[11]
4.9
A number of submissions suggested a range of possible additional
measures to address harmful alcohol consumption and this is dealt with in
further detail below.
Work underway
4.10
The Government has already acknowledged that a range of measures are
required to address harmful alcohol consumption in the community, that this measure
is a first step, and has noted there is significant work already underway in
this area including:
- The National Alcohol Strategy 2006–2009 which was developed
through collaboration between Australian governments, non-government and industry
partners and the broader community. It outlines priority areas for coordinated
action to develop drinking cultures that support a reduction in alcohol-related
harm in Australia;[12]
- The National Binge Drinking Strategy was announced by the Prime
Minister on 10 March 2008. In particular, it announced three measures to reduce
alcohol misuse and 'binge drinking' among young Australians:
- community level initiatives to confront the culture of 'binge
drinking', particularly in sporting organisations;
- earlier intervention to assist young people and ensure they
assume personal responsibility for their 'binge drinking';
- advertising that confronts young people with the costs and
consequences of 'binge drinking';[13]
- On 26 March 2008, COAG asked the Ministerial Council on Drug
Strategy to report to COAG in December 2008 on options to reduce binge drinking
such as: closing hours, responsible service of alcohol, reckless secondary
supply and the alcohol content in RTDs. To acknowledge the urgency required to
address alcohol abuse, this work has now been brought forward to July 2008.[14]
COAG also asked the Australia New Zealand Food Regulation Ministerial Council
to request Food Standards Australia New Zealand to consider mandatory health
warnings on packaged alcohol.[15]
4.11
A comprehensive list of forums considering alcohol issues is available
in the Senate Community Affairs Report on the Alcohol Toll Reduction Bill 2008.
Further measures
4.12
Witnesses reinforced the need to look at additional options to reduce
binge drinking. Submissions suggested a number of areas including:
- packaging/labelling;[16]
- strategically designed education programs on the health and
social harms to reduce consumption;[17]
- ensure uniform laws, involving heavy penalties, on the provision
of alcohol to teenagers;[18]
- law enforcement initiatives;[19]
- legislation to place limitations on the density of liquor outlets;[20]
- control the time limit for purchase of alcohol as well as the
rate/volume purchased;[21]
- modifications to the rules governing advertising, marketing,
promotion, media and sponsorship;[22]
- consideration of the promotional links between alcohol and sport;[23]
- the role of parents as role models and supervisors;[24]
- reducing the allowable alcohol content in RTDs to no more than
three per cent;[25]
- reducing the availability of alcohol;[26]
- raising or gradually raising the drinking age to 21 as by this
age the brain is better protected from brain damage as a result of alcohol
consumption;[27]
and
-
review of alcohol taxation (addressed in more detail below).[28]
4.13
The RACP informed the Committee that an evaluation of international
literature found the following list of nine 'best practices' to deal with
alcohol related problems:
Alcohol control policies
- alcohol taxes;
- minimum legal purchase age;
-
government monopoly of retail sales;
- restriction on hours or days of sale;
- outlet density restrictions.
Drink-driving countermeasures
- sobriety check points;
- lowered blood alcohol content limits;
- administrative license suspension;
- graduated licensing for novice drivers.[29]
4.14
Submissions also mentioned a comprehensive strategy taking into
consideration associated issues such as the role of primary care and the
pressure placed on treatment services for alcohol related issues and workforce
development.[30]
4.15
The question of the responsibility of parents was discussed during the
hearings primarily due to the AIHW finding that among underage drinkers of
RTDs, alcohol is usually sourced from a friend or acquaintance, or from a
parent.[31]
Professor Robin Room, Alcohol and other Drugs Council of Australia, acknowledged
that parents face a difficult task regarding the most appropriate ways to
introduce and control the consumption of alcohol. In response to questions from
the Committee he advised:
I think it is appropriate for a parent to be reminding their
children of the law that applies at least outside their own home. Within their
own home, again, there are going to be differences.[32]
4.16
Professor Michael Moore, Chief Executive Officer, Public Health
Association of Australia, told the Committee that he thought governments could
support parenting by giving them ideas to consider and to that end any
marketing campaign should also reach parents as well as young people. He also
emphasised the significant influence of parents as role models.[33]
4.17
The NDRI noted that Australians are currently more receptive to measures
to address alcohol-related harm. They cited the 2007 National Drug Strategy
Household Survey findings that there has been a significant increase in public
support for changes in alcohol related policy, including support for increasing
the price of alcohol and increasing the tax on alcohol to pay for health,
education and treatment of alcohol related problems.[34]
The issue of hypothecated tax is addressed later in this chapter.
Conclusion
4.18
The Committee notes the consistent argument from witnesses that the
measure to raise the price of RTDs, although a positive step, would be more
effective if it was part of a comprehensive strategy to address the harms
associated with alcohol consumption for not only young and underage drinkers
but all at-risk drinkers. This comprehensive strategy would involve all the stakeholders
and the Committee particularly commends the willingness of industry to be
involved.
4.19
The Committee also notes the government has already acknowledged that a
range of measures will be required to address harmful alcohol consumption. The Committee
commends the work currently underway in this area including the announcement of
the National Binge Drinking Strategy and the targeted work being undertaken for
COAG regarding options to reduce binge drinking with an interim report now due
in July 2008. The Committee is aware that some of the additional measures
raised in evidence to this inquiry will be included through the COAG work but
strongly supports the whole range being considered as part of the review.
4.20
The Committee also supports the work being undertaken for COAG to raise
a proposal to consider mandatory health advisory labels on packaged alcohol. The
Committee is pleased to note the receptiveness of the public to measures to
address alcohol related harm found in the National Drug Strategy Household
Survey and urges the Government to take into consideration the increased public
support for changes in alcohol related policy.
Recommendation 1
4.21
The Committee supports the introduction of the excise increase on spirit
based RTDs, and does so in acknowledgement that it is one in the context of a
range of measures undertaken or to be considered to address harmful alcohol
consumption by young people.
Recommendation 2
4.22
The Committee notes that some of the additional measures suggested to
the Committee will be included in the work being undertaken for COAG but
strongly supports the whole range being considered as part of the review.
Interpreting the data
4.23
Some submissions questioned the conclusions drawn from data from the
AIHW and the NDSH Survey. They suggested the evidential link between increasing
the price of RTDs and a reduction in binge drinking among young women is
tenuous at best. Organisations such as Diageo, Australian Hotels Association, the
Winemakers' Federation of Australia and Wine Grape Growers' Australia pointed
out that overall alcohol consumption fell between 2004 and 2007 and that
between 1991 and 2007 for those aged 14 years or older, alcohol consumption
patterns remained largely unchanged. They contend that there is no evidence to
support the current crisis over the levels of risky drinking of either gender.[35]
4.24
Industry also noted that 75 per cent of RTDs are dark spirits mainly
favoured by men aged 24 years or older[36]
and of the remaining market for light RTDs, they asserted approximately 29 per
cent of the volume was consumed by males.[37]
Conclusion
4.25
The Committee notes some confusion caused by interpretations of data by
various stakeholders and the tendency to highlight minor variations between
individual studies. Despite this debate on data, which will no doubt continue,
there is no mistaking the unanimous conclusion of the health and medical
professionals that there are unacceptably high rates of risky and high risk
alcohol consumption by young people, rising rates of alcohol-related harm and
hospitalisations and increasing social costs.
4.26
The Committee does not accept that there is no evidence for undertaking
the measure to increase the excise on spirit-based RTDs. The Committee acknowledges
the data showing overall alcohol consumption remaining largely unchanged. It
also notes that within this, the drinking patterns and preferences vary considerably
across age and sex as described in the previous chapter. The Committee agrees
there are widespread indicators that young people commonly engage in risky
drinking behaviour at unacceptable levels and that action must be taken to
protect what appears to be a significant proportion of young people from the
harms resulting from drinking to excess.
4.27
The Committee recognises that RTDs are not exclusively consumed by
adolescents and teenagers and they are not the sole alcohol product preferred
by this age group. The Committee notes that the RTD data from industry
understandably does not cover underage drinking and therefore turns to the data
presented in detail in chapter three for this age group. In particular the Committee
notes RTDs are of concern as they are one of the most popular alcoholic
beverages, the most common first-used alcoholic beverage among younger age
groups and are the preferred drink for young people who drink at risky levels.
4.28
In reaching this conclusion the Committee notes data such as the 2006 ASSAD
survey which showed an increasing preference for RTDs among 12 to 17 year old females.
AIHW data also showed a significant increase in the consumption of RTDs. There
was also a clear preference among females in the 16 to 17 age group for
premixed spirits in a can and premixed spirits in a bottle which was the
highest preference for that age group. The NDSHS also showed a strong
preference among females between 12 to 17 for pre-mixed spirits and bottled
spirits. The Committee notes the conclusion from the AMA that this data indicated
'a policy focus on RTDs is justified as part of a total alcohol strategy'.[38]
4.29
The Committee also notes the research on behaviour cited in submissions
such as the NDRI which reported that when adolescents consume alcohol, most do
so at risky levels with 85 per cent of alcohol consumption for females aged 14
to 17 years and 18 to 24 years at risky or high risk levels for acute harm.[39]
More recent data confirmed these findings in a number of studies and surveys
all showing high rates of harmful drinking.[40]
The Committee notes the results from the recent NDSHS indicating that 9.1 per
cent of 14 to 19 year olds (and a greater proportion of girls than boys) drink
at risky or high risk levels at least once a week. The AMA noted that while
this survey did not indicate an increase in risky and high risk drinking in
this age range since 2004, the findings were still a matter for significant
concern due to the increased vulnerability of this age group to the effects of
alcohol and increased risk of harm.[41]
4.30
In addition to drinking preference changes and associated health effects,
the Committee also notes the high levels of harm due to alcohol consumption
outlined in chapter three. The Committee agrees that the current levels of
risky and high risk alcohol consumption by young and particularly underage
drinkers are unacceptably high. The evidence strongly indicates that action
needs to be taken to prevent both the health and social consequences of risky
drinking behaviour in young people.
4.31
The Committee notes that industry has acknowledged the level of public
concern with the voluntary action to reduce the amount of alcohol to two
standard drinks in their RTD products. Despite this voluntary action evidence
from organisations including the Australian Psychological Society contended
that self regulation did not appear to be working.[42]
The Committee notes that the industry acknowledged that reducing the incidence
of intoxication of young people should be a priority area and have shown a
willingness to provide input, work in partnership and be part of the solution.[43]
Potential for substitution
4.32
Submissions noted that the increase in growth of RTDs had come at the
expense of bottled full strength spirits and full strength beer[44]
and that if pre-mixed spirits became too expensive those who wished to binge
drink would move down the alcohol cost curve and simply substitute RTDs with
other, cheaper alcohol. Submissions cautioned that while certain customers may
respond to price increases by altering their total consumption, others would
respond by varying their choice of type or quality.
4.33
Industry sources, including Diageo, noted that one alternative would be
for the customer to purchase a bottle of full strength spirits and use mixers
to make their own RTD which is likely to result in non-standard drinks which
make it difficult to keep track of alcohol consumed.[45]
4.34
AHA agreed that instead of a reduction in alcohol consumption there
would be a shift to other products such as bottles of spirits or beer. They
further stated that an increase in alcohol was a blunt instrument which merely
disadvantaged that product in the market as consumers move to other options.[46]
The Australian Wine Research Institute also cautioned that reductions in sales could
be mitigated by substitution between beverage types.[47]
4.35
To address this issue various groups have called on the Government to
impose a higher uniform tax across all alcohol types to discourage 'drink
hopping'.[48]
Drug Awareness (NSW) also believed there was potential for young people to
switch to other spirits and mix their own drinks and that this highlighted the
need for much higher taxes on all alcohol.[49]
The issue of alcohol taxation is addressed in more detail later in this chapter.
4.36
The NDRI noted the importance of the taxation strategy because where
discrepancies exist, those who seek intoxication at the lowest price may engage
in substitution. However, they noted that it was important to place the issue
of substitution in a wider context as the degree to which this undermined the
overall effect of restrictions on the availability of alcohol was likely to be
limited.[50]
A recent review of alcohol restrictions noted:
A minority of drinkers, retailers and producers will always seek
to find a way around restrictions, but it is nonetheless possible to anticipate
how and where substitution practices may occur and to implement strategies to
limit their impact.[51]
4.37
Professor Robin Room, ADCA, told the Committee that some consumers will
switch to another alcoholic beverage which is cheaper but it won't be a
complete switch. He summarised:
You certainly will be able to find people who will say, 'Now I
drink something else.' But that does not mean that the tax has not had an
effect. It is very likely to have some kind of effect, partly on ground of
taste and partly on grounds of whatever choices people make in their lives.[52]
4.38
Professor Michael Moore, PHAA, acknowledged the potential for
substitution but told the Committee:
The fundamental question we are asking is: how can we reduce the
level of harm associated with heavy drinking of alcohol? And, fundamentally, it
comes back to a cost-benefit analysis that says that, even though some people
will move to hard spirits, we believe that this first step on the taxation of
these particular drinks is likely to reduce harm overall and that a more
comprehensive approach will be much more effective in reducing the harmful use
of alcohol. We see this as a good first step, but only as a first step.[53]
4.39
Regarding the potential for substitution Professor Steve Allsop, NDRI, advised
monitoring and pointed out to the Committee that mixing your own drinks was
already a cheaper option available to young people prior to the increase in
taxation.
Even before the increase in taxation, it was cheaper to buy a
bottle of spirits and to buy your own mixer. So it was not a widespread
practice then; there is no evidence that it will become a widespread practice
subsequently.[54]
4.40
Dr Tanya Chikritzhs, NDRI, emphasised that substitution effects are to
some degree inevitable but:
The overall finding for all of the studies that we have been
able to review is that the substitution effects are minimal compared to the
overall benefits that are brought about by the restrictions.[55]
4.41
Dr Alexander Wodak, RACP, told the Committee that a small proportion of
the population consumed a disproportionate amount of the alcohol consumed in the
community and concluded:
When we have relatively small changes in availability or price
relative to income, we have large changes in consumption, with a lot of that
consumption accounted for by people drinking immoderately and therefore
exposing themselves and other to great harm.[56]
4.42
Ms Virginia Hart, Assistant Secretary, Drug Strategy Branch, Department
of Health and Ageing told the Committee during estimates hearings that they were
in the process of designing an evaluation for all components of the binge drinking
strategy and also the increase in excise.[57]
At the hearing the department reinforced that:
...the RTD excise is only one lever being used to tackle
adolescent binge drinking. We are in the process of now trying to devise an
evaluation to look at how all the initiatives that we have set out will
contribute to tackling binge drinking.[58]
Recommendation 3
4.43
The Committee notes the potential for alcohol substitution to occur and supports
the government's commitment to evaluate the effectiveness of the measure
increasing the excise on spirit-based RTDs and all components of the binge
drinking strategy.
Conclusion
4.44
The Committee acknowledges the potential for substitution of RTDs with
other alcoholic beverages, particularly by those whose sole purpose is to become
intoxicated. The Committee notes the data released by DSCIA over a two week
period which may indicate a tendency for this to occur for some consumers but
concludes the timeframe is too short to draw meaningful conclusions. The Committee
also notes the evidence by organisations such as the NDRI that the degree to
which substitution undermines the overall effect of restrictions on the
availability of alcohol is likely to be limited. The Committee was also
cognisant of international data outlined in chapter three which appears to
support this. The Committee supports the government's plan to evaluate the
increase in excise and urges the government consider additional strategies as required.
Alcohol taxation issues
4.45
The majority of submissions drew attention to the anomalies that existed
in the alcohol taxation system, which do not help to achieve good health policy
outcomes and called for these inconsistencies to be addressed.
4.46
Below is a detailed description of the current tax system by DSICA:
All categories of alcohol are subject to the GST at the general
rate of 10 per cent. In addition to the GST, wine, beer and spirits are subject
to different Commonwealth alcohol taxation regimes. Beer, spirits and
ready-to-drink alcohol beverages below 10 per cent alcohol content are subject
to excise or customs duty. Australian produced beer, spirits and pre-mixed
products are subject to excise duty, collected by the Australian Taxation Office.
Imported beer, spirits and pre-mixed spirit products are subject to customs duty
collected by the Australian Customs Service. However, imported spirits and
pre-mixed spirits (but not beer) are also subject to an additional 5 per cent
ad valorem customs duty, or protective tariff. Excise duties and customs duties
(excluding the 5 per cent ad valorem tariff) are set on a volumetric basis, ie.
levied on the actual amount of alcohol in the product. Excise duty and the
volumetric component of the customs duty are set at the same level for each
alcohol category, and are automatically increased twice a year (1 February and
1 August) to take account of movement in the consumer price index in the
previous six months. All wine (including cask and bottled wine, other grape
wine products such as marsala and vermouth, mead and sake, and traditional
cider) is subject to the Wine Equalisation Tax (WET). WET applies at the rate
of 29 per cent of the last wholesale selling price (usually the last sale from
the wholesaler to the retailer). The taxation of wine differs to the tax
situation in relation to beer, spirits and ready-to-drink products in two
significant ways. Firstly the WET is levied on an ad valorem basis (ie. a tax
on value) rather than on the alcohol content of the product. Secondly, there is
no automatic six monthly indexation of the WET as there is for spirits and
beer.[59]
4.47
The majority of submissions called for a comprehensive review and reform
of alcohol taxation. The overwhelming view from public health advocates and some
elements of industry was that alcohol taxation should be largely based on
alcohol content and as much as possible this should be true within and between
beverage classes. Submissions argued that from a public health perspective,
there was no basis to discriminate between alcohol beverages.
4.48
The National Drug Research Institute (NDRI) noted that:
The most effective taxation strategy to prevent and reduce
alcohol related problems is one where all alcoholic beverages are taxed
according to their alcohol content.[60]
4.49
The Alcohol Education and Rehabilitation (AER) Foundation welcomed the Government's
move to tax RTDs at the same volumetric rate as bottled spirits as the first
step to a fairer alcohol taxation system. The CEO, Daryl Smeaton, urged that
further action needed to be taken to address taxation inconsistencies around
products such as cask wine, cheap fortified wines such as port and full
strength beer which continued to have advantageous tax rates and has urged the
government to undertake a full alcohol taxation review.[61]
AER proposed that all alcohol products should be taxed according to the amount
of alcohol contained in the package:
Imposing a consistent tax by volume regime across all beverage
types will help change the consumption patterns that lead to binge drinking in
both young and old.[62]
4.50
The Australian Drug Foundation also called for a volumetric based
taxation regime, arguing that the current system facilitated the sale of
high-alcohol products at cheap prices.[63]
The volumetric approach was also supported by the Public Health Association of
Australia[64]
and Independent Distillers Australia[65]among
others.
4.51
The NDRI suggested a tiered volumetric tax where the base tax was
determined according to alcohol content and an additional 'harm index' was
applied to beverages shown to be particularly problematic and/or associated with
high levels of harm.[66]
4.52
Higher taxes on strong beverages was supported by Professor Robin Room
who suggested the general principle of 'taxing according to the volume of pure
alcohol in the beverage and setting taxes high enough to mildly discourage
consumption'.[67]
He advocated modification of these general principles in the following ways:
- a higher tax for strong beverages of 20 per cent alcohol and
higher to reflect the much greater possibility of overdose from these
beverages;
- a lower tax for weak beverages below 3.5 per cent to encourage
switching to low-alcohol beverages;
- a higher tax to respond to problematic fashions and social trends
such as beverages favoured by young binge drinkers; and
- the imposition of a minimum price level on each type of beverage
which particularly affects underage and heavy drinkers.[68]
4.53
Ms Kate Carnell, AGPN, suggested an escalation approach which has
incentives for industry to produce low-alcohol products with under 3.5 per cent
alcohol.[69]
4.54
Those industry groups which modelling shows would be most advantaged
strongly supported a volumetric tax. Diageo also described the current tax
system as unnecessarily complex and called for volumetric tax as the most
effective, efficient and equitable way to tax alcohol as:
The effect on the body is the same whether the alcohol is
consumed from a beer, a wine or a spirit.[70]
4.55
DSICA contended that the current different types and rates of taxation did
not achieve positive social and health and outcomes and would add to the issue
as it provided stronger incentives to produce and consume alternative and
cheaper beverages.[71]
4.56
The AER told the Committee a comprehensive review of the alcohol
taxation system is required as:
It is broken. It is unfair. It is inconsistent. And it does not
tax alcohol as alcohol. It taxes beverages according to the way they are made;
and, of course, in the case of wine, according to the value put on that wine by
the manufacturers.[72]
4.57
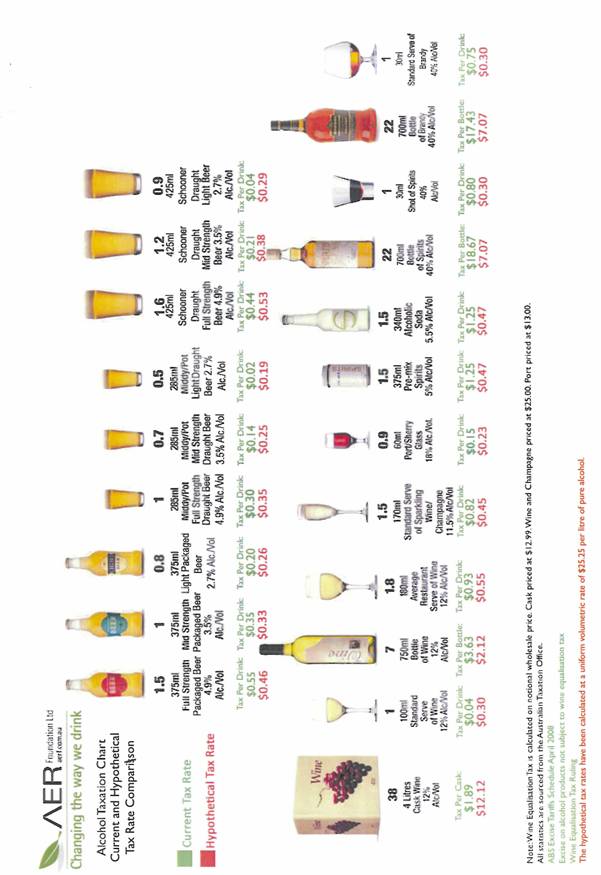
Modelling was provided by the AER[73]
(see diagram below) which shows volumetric taxation would mean significant
changes for the industry. It shows a hypothetical tax rate calculated at a
uniform volumetric rate of $25.25 per litre of pure alcohol.
4.58
Mr Daryl Smeaton, Chief Executive Officer AER, emphasised the modelling
was not a recommendation but an example of what a single rate of taxation would
look like that produced revenue neutrality and reduced consumption. He added:
I think there are a whole range of models that should be looked
at, but they must all have one fundamental element to them—that is, they must
tax the alcohol as alcohol and not as wine, beer or spirits. There is no
difference in the alcohol in beer or wine or spirits in terms of the potential
harm its excessive consumption can cause. That is the fundamental reason for a
comprehensive review of the taxation system. It should not be based on how the
product is made, who makes it or what its economic benefits or disbenefits are;
it should be reviewed from a public health perspective. This is an industry
that gets $30 billion a year in alcohol sales and that creates, on a very
conservative estimate, $15.3 billion worth of harm—and we think that is a very
conservative estimate.[74]
4.59
The Brewers Association for Australia and New Zealand provided the
Committee with independent modelling from Access Economics on volumetric
taxation which found that this system would result in the fall of prices of all
spirits and beer and wine prices would rise. On this basis the association
submitted that there were industry, agriculture and health policy reasons to reject
volumetric taxation as compared to the range of spirits and wine products, 'all
beer is low alcohol'.[75]
4.60
The rejection of volumetric taxation was supported by the Winemakers' Federation
of Australia and Wine Grape Growers' Australia which argued that taxation was a
blunt instrument which did not distinguish between responsible and harmful
drinking. They contended that wine was not attractive to younger drinkers and
therefore not the product of choice for most underage drinkers.[76]
This was observed in the data from the AIHW where it was shown that this change
in drinking pattern picked up when consumers reached their twenties.[77]
A number of submissions, however, called for measures to address harmful
alcohol consumption in all age groups.
4.61
The wine sector also noted that any measures to increase taxation in the
wine sector or change the way the product is taxed would have a negative effect
on employment and regional communities which were already dealing with the
challenges associated with the drought and water prices.[78]
4.62
When speaking to the Committee Mr Stephen Strachan, Chief Executive,
Winemakers' Federation of Australia, highlighted the following effects of a
volumetric tax for the wine industry:
A uniform volumetric tax at, say, the beer rate would lead to an
increase in the price of a $12.50 cask of wine to $28; an increase in price for
all bottled wine that currently sells below $25, which accounts for about 98
per cent of all the wine that we sell in Australia, including cask wine; a
reduction in wine demand, resulting in a drop of about 250,000 tonnes of grapes
required by the industry for the domestic market; and about 3,500 fewer
employees—in terms of the people who are employed by that part of the business.
It would also of course result in a drop in the price of spirits and would
result, at the beer rate, in a modest drop in government taxation revenue,
although it would be very modest. A revenue neutral volumetric type tax across
all alcohol would necessarily be slightly higher than the beer rate, and that
would obviously lead to even more pronounced impacts on the wine industry.[79]
4.63
While sensitive to the concerns of industry, in response to questioning
from the Committee on the effect of volumetric taxation on the wine industry, Professor
Richard Mattick, Director, National Drug and Alcohol Research Centre, told the
Committee:
I think you have to think about what the severity of the impact
might be. The example given here was that a 10 per cent increase might affect
consumption by less than 10 per cent. It is not stopping five per cent of
people drinking; it is reducing consumption overall by five per cent, and that
is the desired effect. A five per cent reduction in consumption would be, I
would suggest, something that the industry could bear. It has seen good growth
over time. One has to ask: does the industry have the unbridled right to grow
and complain when anybody calls attention to this issue and calls foul, or are
we thinking, ‘Hang on, the consumption in Australia is getting to be high’—and
it has been high for a long time—and thinking about some reasonable measures
which respect the industry’s right to continue to employ and to produce? Also,
the industry makes a lot of money by exporting overseas, and presumably some of
these tax measures will not be affecting it there. But I still think that the
government needs to have some control over consumption.[80]
4.64
Dr Anthony Shakeshaft, Senior Lecturer, National Drug and Alcohol
Research Centre, argued that a volumetric taxation system would provide the opportunity
for industry to better align with public health goals:
From a public health perspective, what we want to see is an
overall reduction in average consumption—how much people drink all the time—as
well as a reduction in how much people drink on one occasion. That is the idea
of the long-term harm as opposed to the short-term harm. We think once you take
out the price differential, then there is an opportunity to get the industry to
compete on things other than price that, as I said, would align better with
public health. For example, you could get them to promote things like lower
alcohol beverages. They could compete to increase in their market share on
issues that use those kinds of strategies rather than just on price.[81]
4.65
Ms Karen Price, Manager of Operations and Development, National Drug and
Alcohol Research Centre, emphasised that aligning public health goals with
industry goals would be the optimal outcome. She stated:
Part of the reason that it [data] is tricky and confusing is
that you have two different groups telling you different messages because they
have different goals. You should have them swinging behind the same goal, and I
think a taxation discussion about alcohol should be about that.[82]
4.66
On the issue of alcohol taxation, the Department of Health and Ageing
stated that in the context of harm minimisation:
there is support for a tax system that provides incentives for
the production, sale and consumption of lower alcohol content beverages and for
using taxation and price to maximise harm minimisation outcomes. The evidence
indicates this can have the impact of reducing overall alcohol consumption and
correspondingly reducing related problems for individuals and communities.[83]
4.67
While supporting a move towards a volumetric tax, Dr Alexander Wodak,
RACP, cautioned that the tax relief for low-alcoholic beverages should not be
removed.[84]
Hypothecated tax
4.68
A number of submissions strongly advocated spending more of the alcohol
profits on education programs and public health campaigns to encourage everyone
to drink safely. Submissions also suggested directing a proportion of the
revenue collected from taxes on alcohol towards funding the Government's
response to the health, social and economic harms resulting from alcohol
misuse. The RACP noted that this measure had been shown to reduce the level of
alcohol-related harm.[85]
This was also supported by organisations including the AMA[86],
the Royal Australasian College of Physicians[87],
the Australian Drug Foundation,[88]
the Australasian Therapeutic Communities Association,[89]
and the Victorian Alcohol and Drug Association[90]
among others.
4.69
Witnesses at the hearing also spoke strongly about the benefits of a
hypothecated tax. Professor Room, ADCA, told the Committee:
It makes sense to use part of these revenues [from alcoholic
beverages] for prevention and treatment programs aimed specifically at alcohol
problems. Such programs should be based on evidence about what is effective and
cost-effective. The rest of the revenues might well be used to support general
health and social welfare services. Alcohol consumption places great burdens on
these systems in terms of emergency department visits, hospital admissions,
family welfare and child protection assistance and so on. The revenues from
increased alcohol taxes would go some way toward paying for these externalities
which alcohol consumption imposes on Australian society.[91]
4.70
The Public Health Association believed that government recognition
should be given to the revenue from the excise increase to be used as part of a
complete package to address the problem and that the funds raised should go
towards 'a comprehensive approach to harmful and hazardous use of alcohol'.[92]
4.71
At the hearing the Ms Jennifer Bryant, First Assistant Secretary,
Population Health Division, Department of Health and Ageing told the Committee
that:
Minister Roxon has stated on the public record that the
government will be looking to direct a substantive proportion of the funds
raised through the excise measure to preventative health activities. Exactly
what those activities will be is still a matter for decision by government...[93]
Conclusion
4.72
The Committee notes the concerns about using tax to control alcohol
consumption as well as the call to tax alcohol content equally, regardless of
product. The Committee also recognises that the support for volumetric taxation
is not unanimous and notes the differing modelling submitted to the Committee. The
Committee fully supports the inclusion of the examination of alcohol taxation in
the current review of the taxation system being chaired by Mr Ken Henry.[94]
4.73
The Committee notes that although wine is a product of choice for an
older age group, this would not deter those whose prime motivation is drinking
to become intoxicated. The Committee also notes the wine industry concerns
regarding potential changes to the alcohol taxation system and urges the
government to take these concerns into consideration during the examination of
alcohol taxation.
Recommendation 4
4.74
The Committee supports the call for a review of alcohol taxation and
notes that an examination of alcohol taxation will be included in the
comprehensive review of the tax system currently underway (the Henry Review).
Other issues
4.75
The Committee noted the submission from the Chrisco Group which raised
the effect of the excise increase on retailers which have pre-sold RTDs at a
fixed price established prior to the increase in the excise.[95]
Conclusion
4.76
The Committee is of the view that the measure undertaken by the Government
to increase the excise on spirit-based RTDs, and this inquiry, have contributed
to the important debate of the role of alcohol in society and the negative
effects of harmful consumption, particularly for young people. The Committee is
aware of and shares the high level of public concern regarding the unacceptable
rates of risky and high risk alcohol consumption of young and underage
drinkers. Young people are particularly vulnerable to alcohol in terms of its effect
on their development, their lack of experience of drinking and the increased
likelihood to engage in risky behaviour which may result in their harm or the
harm of others. The Committee recognises that the vast majority of submissions from
researchers, health and medical professionals supported raising the excise as a
significant step to address this public health issue.
4.77
While some evidence focussed on the drinking patterns of older males and
RTDs the primary aim of the Committee was the effect of alcohol on the short
and long term health of young people. The Committee acknowledges data which
shows the relatively stable consumption patterns for people aged 14 years or older;
however, it also recognises that within this data, drinking patterns and
preferences vary considerably across age and sex. The evidence shows a
widespread problem with the illegal consumption of alcohol by underage
drinkers. Evidence also shows that a significant proportion of underage
drinkers are risking harm to themselves and others by engaging in risky
drinking behaviour.
4.78
There has been a growth in new alcohol products over recent years and
the Committee notes the significant growth in the consumption of RTDs and that they
are being consumed at risky and high risk levels by young drinkers. While this
increase may have been at the expense of other alcoholic beverages there is no
denying the attractiveness of RTDs for young and underage drinkers. They are
often their first drinks, their most preferred, they mask the taste of alcohol
which makes them palatable to very young drinkers, have colourful packaging and
a relatively high alcohol content for those whose objective is rapid
intoxication. Young females in particular display a preference for sweet
tasting and colourful RTDS. The Committee agrees that measures need to consider
the drinking preference of at-risk adolescents and teenagers where evidence
indicates that RTDs are particularly appealing.
4.79
The data from surveys and studies shows young females have stronger
preferences for pre-mixed drinks in a can or bottle when compared to young
males. Across a number of surveys RTDs have become more popular, showing a
substantial increase in consumption, particularly among young girls. However,
the Committee notes the figures are concerning for both sexes. The
attractiveness of RTDs is also evident in the sales figures with an increase of
more than 450 per cent between 1997 and 2006.
4.80
The Committee notes some confusion caused by interpretations of data by
various stakeholders and the tendency to highlight minor variations between
individual studies. Despite this debate, which will no doubt continue, there is
no mistaking the unanimous conclusion of the health and medical professionals
that there are unacceptably high rates of risky and high risk alcohol
consumption by young people and rising rates of alcohol-related harm and
hospitalisations.
4.81
The Committee agrees there are widespread indicators that young people
commonly engage in risky drinking behaviour at unacceptable levels and that
action must be taken to protect what appears to be a significant proportion of
young people from the harms resulting from drinking to excess.
4.82
The level of public concern has been recognised by the industry itself
as evidenced by the voluntary action taken to reduce the amount of alcohol to
two standard drinks in their RTD products in response to the level of concern.
Despite this voluntary action the Committee notes evidence that this appears to
be having minimal effect, however, the Committee commends the willingness of
industry to be part of the solution.
4.83
Evidence clearly demonstrates the high levels of risky and high risk
drinking behaviour and the consequences of this can be found in ongoing
negative health effects, including motor accidents and hospitalisations. The
data on treatment episodes, preventable health problems, deaths and hospitalisations
all clearly show unacceptable increases for young people. These health findings
alone justify the measure undertaken by the government. In addition to the
negative health effects, evidence also shows an increase in the levels of
sexual assaults, physical violence and criminal activity which affects not only
the young people involved but also the broader community.
4.84
The Committee agrees that the current levels of risky and high risk
alcohol consumption by young and particularly underage drinkers are
unacceptably high. The evidence strongly indicates that action needs to be
taken to prevent both the health and social consequences of risky drinking
behaviour in young people.
4.85
The effect of alcohol taxes on risky and high risk alcohol consumption
by young and underage drinkers is a complex question and the Committee
acknowledges the potential for drink substitution to occur. DSICA put forward
data collected over a two week period to support this argument. However, the Committee
concludes that the timeframe is too short to draw meaningful conclusions. The Committee
also notes the evidence by NDRI and others which argued that the degree to
which substitution undermined the overall effect of restrictions on the
availability of alcohol was likely to be limited. Therefore, the Committee
urges the government to monitor and evaluate this aspect and consider additional
strategies as required.
4.86
The Committee notes the consistent argument from witnesses that while
supportive of the measure to raise the price of spirit-based RTDs it would be
more effective as part of a comprehensive approach to address the harms
associated with alcohol consumption by young and underage drinkers. The Committee
notes the government has already acknowledged that a range of measures are
required to address harmful alcohol consumption in the community through the
implementation of the National Binge Drinking Strategy and looks forward to the
outcomes of the targeted work being undertaken for COAG regarding further options
to reduce 'binge drinking' due in July 2008. The Committee is aware that some
of the additional measures raised will be included through the COAG work but
strongly supports the whole range be considered as part of the review. In
formulating any additional measures, the Committee urges the government take
advantage of the increased public support for changes in alcohol related policy
to address alcohol related harm found by the National Drug Strategy Household
Survey.
4.87
The inquiry has also highlighted the inconsistencies in the current
alcohol taxation system. The Committee acknowledges the concerns about using
tax to control alcohol consumption as well as the call to tax alcohol content
equally, regardless of product. The Committee recognises the call for
volumetric taxation was not universal and there were variations between a flat
or tiered level of taxation by its advocates. The concerns expressed by the
wine industry and the suggestions for exemptions and modelling provided were
noted by the Committee. The Committee supports the examination of alcohol
taxation being included in the Henry review of the taxation system and urges
government to consider the concerns raised and the evidence for and against
volumetric taxation submitted to the inquiry.
4.88
The public health issues of problematic drinking among young people are
clear and each action that reduces such drinking makes a contribution in public
health terms. For all the reasons listed above the Committee agrees with the
vast majority of evidence presented to the Committee, particularly by health
and medical professionals, which was supportive of the measure to increase the
price of spirit-based RTDs as one of a range of measures to address harmful
alcohol consumption in the community and particularly among young people. The Committee
notes this is a complex issue and one that will require further effort and
input from governments, professional bodies, researchers, treatment and
prevention services, media, industry and the community to develop the next
steps.
Senator Claire
Moore
Chair
June 2008
Navigation: Previous Page | Contents | Next Page