Introduction
Establishment
1.1
On 11 October 2016, the Senate established the Select Committee on Red
Tape (committee) to inquire into and report on the effect of restrictions and
prohibitions on business (red tape) on the economy and community, by 1 December
2017, with particular reference to:
- the
effects on compliance costs (in hours and money), economic output, employment
and government revenue, with particular attention to industries, such as
mining, manufacturing, tourism and agriculture, and small business;
- any
specific areas of red tape that are particularly burdensome, complex, redundant
or duplicated across jurisdictions;
- the
impact on health, safety and economic opportunity, particularly for the
low-skilled and disadvantaged;
- the
effectiveness of the Abbott, Turnbull and previous governments' efforts to
reduce red tape;
- the
adequacy of current institutional structures (such as Regulation Impact
Statements, the Office of Best Practice Regulation and red tape repeal days)
for achieving genuine and permanent reductions to red tape;
- alternative
institutional arrangements to reduce red tape, including providing subsidies or
tax concessions to businesses to achieve outcomes currently achieved through
regulation;
- how
different jurisdictions in Australia and internationally have attempted to
reduce red tape; and
- any
related matters.[1]
1.2
On 28 November 2017, the Senate extended the reporting date to 3
December 2018.[2]
1.3
The committee decided to conduct its inquiry by focusing on specific
areas. This interim report presents the committee's findings and conclusions
about the effect of red tape on health services (health services inquiry).
Conduct of the health services inquiry and acknowledgement
1.4
The committee advertised the health services inquiry on its website and
wrote to a number of organisations, inviting submissions by 22 January 2018. The committee
continued to accept submissions received after this date. In total, the committee
received 11 submissions, which are listed at Appendix 1.
1.5
The committee held a public hearing in Canberra on 9 February 2018. The witnesses
who appeared before the committee are listed at Appendix 2.
1.6
The committee thanks the organisations who made submissions and who gave
evidence to assist the committee with its health services inquiry.
Scope of the report
1.7
Chapter one provides broad background information to set the regulatory
context for the health services inquiry. Chapter two then examines some of the information
presented to the committee, which may be drawn upon in the committee's final
report.
Regulatory framework for health services
1.8
The health services inquiry encompasses Commonwealth, state, territory
and local government responsibilities. Accordingly, there are a number of
regulatory regimes upon which submitters and witnesses could comment. In this
report, the committee focussed primarily upon Commonwealth responsibilities.
Figure 1 illustrates the responsibilities of each level of government.
Figure 1.1: Government responsibilities, Australian
health system
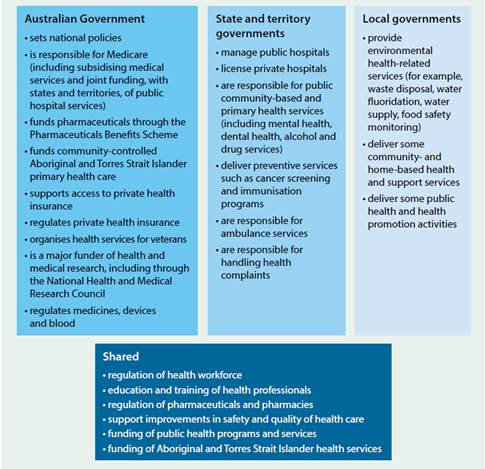
Source: Australian Institute of Health and Welfare,
Australia's Health 2016, 2016, p. 24.
Australian Government responsibilities
1.9
The Department of Health (Department) has a diverse range of
responsibilities which reflect a common purpose—better health and ageing
outcomes for all Australians.[3]
In total there are 10 outcomes including: access to medical and dental services;
primary health care; private health; and health infrastructure, regulation,
safety and quality. Specific agencies—such as the Australian Commission on
Safety and Quality in Health Care and the National Health and Medical Research
Council—are responsible for a further 20 outcomes in the Health portfolio.[4]
Regulatory Reform Agenda
1.10
In 2013, the Australian Government introduced the Regulatory Reform
Agenda (Agenda): to reduce the burden of regulation across government;
to coordinate red tape reduction efforts; and to set clear expectations
that regulation should not be the default option for government policy makers.[5]
1.11
Key elements of the Agenda include:
-
cutting regulatory compliance costs to businesses, community
organisations and individuals by at least $1 billion a year;
-
requiring all major regulatory decisions to be informed by a Regulation
Impact Statement (RIS) that sets out the benefits/costs of regulation;
-
introducing the Regulatory Burden Measurement framework to
calculate the regulatory costs of current/proposed policies or regulation;
-
undertaking an assessment of the regulatory burden imposed by the
Commonwealth stock of regulation; and
-
introducing the Regulator Performance Framework for over 80
regulatory authorities, to encourage regulators to:
-
reduce regulatory burden;
-
communicate clearly with stakeholders;
-
take risk‑based and proportionate approaches to regulation;
-
operate efficiently and transparently; and
-
undertake continuous improvement.[6]
Performance under the Regulatory
Reform Agenda
1.12
By 31 December 2015, the Australian Government reported having made
decisions to reduce regulation compliance costs by $4.8 billion.[7]
Of this total, the Department reported it had achieved net savings of $249
million, with significant reductions in red tape, notwithstanding the
introduction of new regulation.[8]
1.13
The Department of the Prime Minister and Cabinet (PMC), which is
responsible for coordinating the regulatory policy priorities across all
portfolios, has not published up‑to-date information for 2016, 2017
or 2018.[9]
The Department was not able to advise its regulatory savings since 2015, instead
referring the committee to PMC.[10]
1.14
In addition to regulatory savings, the Department advised that it
continually tests the relevance and effectiveness of existing regulation, and
explores opportunities to reduce red tape.[11]
A major deregulatory measure was the 2015 Review of Medicines and
Medical Devices Regulation. This review focussed on the regulatory
framework and processes of the Therapeutic Goods Administration.[12]
1.15
As part of best practice regulation, the Department also conducts
regulatory impact analysis in the form of RISs.[13]
In 2014–2015, six statements were developed, however it is not clear from the
Department's website if any RISs have been developed since 2015.[14]
Navigation: Previous Page | Contents | Next Page